Download
1 / 34
350 likes | 539 Views
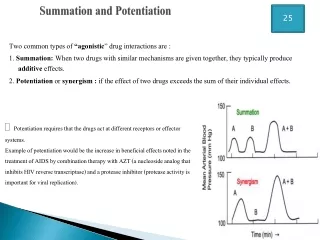
25. Summation and Potentiation. Potentiation requires that the drugs act at different receptors or effector systems.

E N D
25 Summation and Potentiation • Potentiation requires that the drugs act at different receptors or effector systems. Example of potentiation would be the increase in beneficial effects noted in the treatment of AIDS by combination therapy with AZT (a nucleoside analog that inhibits HIV reverse transcriptase) and a protease inhibitor (protease activity is important for viral replication). Two common types of “agonistic” drug interactions are : 1. Summation: When two drugs with similar mechanisms are given together, they typically produce additive effects. 2. Potentiation or synergism : if the effect of two drugs exceeds the sum of their individual effects.
Receptor Theory 1)Receptors largely determine the quantitative relations between dose or concentration of drug and pharmacologic effects 2)Receptors are responsible for selectivity of drug action 3)Receptors mediate the actions of pharmacologic agonists & antagonists
The first step in drug action on specific receptors is the formation of a reversible drug-receptor complex, the reactions being governed by the Law of Mass Action Where [D] = concentration of free drug; [DR] = the concentration of bound drug; [RT] = the total concentration of receptors; kd = the equilibrium dissociation constant and represents the concentration of free drug at which half-maximal binding is observed
Relationship of binding to effect • The binding of a drug to its receptor initiates events that ultimately lead to a measurable biologic respons • The magnitude of response is proportional to the amount of receptors bound/occupied according to the following equation: E = Emax × [D] [D] + EC50 Where [E] = is the effect observed at concentration [D], Emax is the maximal response that can be produced by the drug; and EC50 is the concentration of drug that produces 50% of maximal effect
Drug receptor interaction • The tendency of the a drug to bind to its receptor is governed by its affinity. • The equilibrium dissociation constant (kd) [k-1/k+1] characterizes the receptor affinity for binding the drug in a reciprocal fashion i.e. a high affinity means a small kd • The ability of a drug , once bound, to activate a receptor and generate response is denoted by its efficacy: a drug with high efficacy eliciting, at some concentration, a full response
G-Proteins coupled receptors (GPCRs) • GPCRs are comprised of a single polypeptide chain that has seven membrane-spanning transmembrane) regions • GPCRs couple to a family of heterotrimeric GTP-binding regulatory proteins termed G proteins signal transducers) • The G protein heterotrimer is composed of three subunits:α, β, and γ
The activated G-protein changes the activity of an effector (E) element, usually an enzyme or ion channel. • This effector then changes the concentration of the intracellular second messenger.
Pharmacodynamics • When the drug blocks a receptor, it is known as antagonist and therefore blocks the action of the endogenous transmitter (i.e. it will prevent the natural chemical from acting on the receptor).However, as most drug binding is reversible, there will be competition between the drug and the natural stimulus to the receptor. • The forces that attract the drug to its receptor are termed chemical bonds and they are : (a)hydrogen bond (b) ionic bond (c) covalent bond (d) Vander waals force. • Covalent bond is the strongest bond and the drug-receptor complex is usually irreversible.
Pharmacodynamics • K1 K3 • D+R DR Biological effect • K2 • Where D = Drug, R= receptor DR= Drug receptor complex (affinity) • K1 = association constant • K2 = dissociation constant • K3 = intrinsic activity
When first messengers like neurotransmitters, hormones, and most of drugs bind with their specific receptors, the drug receptor complex is formed which subsequently causes the synthesis and release of another intracellular regulatory molecule termed as second messengers e.g. cyclic AMP, calcium, cyclic GMP, inositol triphosphate (IP3), diacylglycerol and calmodulin which in turn produce subcellular or molecular mechanism of drug action
Basics of Drug Action • Desired action – the expected response of a medication • Side effects –known and frequently experienced, expected reaction to drug. • Adverse reaction –unexpected, unpredictable reactions that are not related too usual effects of a normal dose of the drug.
Therapeutic Action • The intended action of a drug given in an appropriate medical setting • Therapeutic Threshold • The minimum amount of a drug that is required to cause the desired response • Therapeutic Index • The difference between the therapeutic threshold and the amount of the drug considered to be toxic • Often referred to as Safe and Effective range
Potentiation • The enhancement of a drug’s effect by another drug Eg. promethazine may enhance the effect of morphine; also alcohol and barbiturates • Refractory • The failure of a patient to respond as expected to a certain medication • Synergism • The combined action of 2 or more drugs that is greater than the sum of the 2 drugs acting independently
Hypersensitivity • A reaction to a drug that is more profound than expected and which often results in an exaggerated immune response • Idiosyncrasy • A reaction to a drug that is significantly different from what is expected • Indication • The medical condition for which the drug has proven therapeutic value
Important Pharmacological Terms • Antagonism • The opposition between 2 or more medications ex. narcotics and Naloxone • Bolus • A single, often large dose of a drug. Often the initial dose • Cumulative action • An increased effect caused by multiple doses of the same drug. Caused by buildup in the blood.
Pharmacotherapeutics • Is defined as the use of drugs to treat diseases. • Depends on: • Severity • Urgency • Prognosis of patient’s condition
1: Enteral Medications • Administered directly into the G.I.T. through the oral, nasogastric (NG) or rectal routes • Advantages: • Convenience for nurse & patient • Most medications are available in oral route • Inexpensive to make oral preparations • Can be removed by gastric lavage or make to vomit
Disadvantages • cannot be administered to very nauseated/vomiting or unconscious persons • some loose their effectiveness if mixed with gastric secretions • onset of action may vary due to changes in absorption in the GIT
Forms of Oral Medication • Capsules-are gelatin containers that hold powder or liquid medicine. • Elixirs- clear liquids made up of drugs dissolved in alcohol & water with coloring & flavoring agents added. • Emulsions-are solutions that have small droplets of water & medication dispersed in oil, or oil & medication dispersed in water.
Forms of Oral Medication • Lozenges- are medicines mixed with a hard sugar base to produce a small, hard preparation of various shapes & sizes. • Suspensions- are liquids with/solid, insoluble drug particles dispersed throughout.
Forms of Oral Medication • Syrups-are liquids w/ a high sugar content designed to disguise the bitter taste of a drug. Pediatric use. • Tablets-dried, powdered drugs compressed into small shapes.
2.Parenteral Administration • Reasons: • When the patient cannot take an oral medication • When the medication must be given quickly • When medication might be destroyed by gastric enzymes • When medication must be given at a controlled rate • When the medication is not available in an enteral form.
Parenteral Medications • INTRAMUSCULAR – 90 ° • Provides faster medication absorption because of muscle’s greater vascularity • SUBCUTANEOUS- 45 ° • Placing medications in the loose connective tissue under the dermis • INTRADERMAL- 15 °
Other Routes of Administration • Topical administration – skin • Cleanse • Soften • Disinfect • Lubricate • E.g. clotrimazole –cream dermatophytosis • atropine- eye-dilate the pupil • Transdermal route - nitroglycerin (skin patch) systemic vasodilation in angina
Other Routes of Administration • Inhalation – provides rapid delivery of drugs to a large area of mucus membranes & tissues of the respiratory system. • Anesthesia • Bronchodilators • Intranasal – desmopressin for diabetes insipidus • Calcitonin- a peptide hormone for tx of osteoporosis
Other Routes of Administration • Intrathecal injection- introduction of hypodermic needle into the subarachnoid space for the purpose of instilling a material for diffusion throughout the spinal fluid. • Intraventricular- space into the ventricle • Both gains access to the CSF e.g. amphotericin B –in meningitis
Rational dosage design • Is based on the assumption that there is a target concentration that will pro duce the desired therapeutic effect • The intensity of a drug's effect is related to its concentration above a minimum effective concentration, whereas the duration of this effect reflects the length of time the drug level is above this value • By considering drug’s PKs, it is possible to individualize the dose regimen to achieve the target concentration