Download

1 / 38
380 likes | 527 Views
2011/9/9. 1. Nagasaki University Hospital established in September 20, 1861. 2011/9/9. 2. Fungus diseases in literature 150 years ago. Okudaira M, Jpn J Pathology : 74, 61-91, 1985. IUMS 2011,Sapporo, JAPAN. Respiratory Mycoses Pulmonary Aspergillosis: Pathogenesis and Treatment

E N D
2011/9/9 1 Nagasaki University Hospital established in September 20, 1861
2011/9/9 2 Fungus diseases in literature 150 years ago Okudaira M, Jpn J Pathology: 74, 61-91, 1985
IUMS 2011,Sapporo, JAPAN Respiratory Mycoses Pulmonary Aspergillosis: Pathogenesis and Treatment Chronic pulmonary aspergillosis ~new treatment evidence and emergence of azole-resistant Aspergillus fumigatus in Japan~ Department of Molecular Microbiology and Immunology Nagasaki University Graduate School of Biomedical Sciences Koichi IZUMIKAWA, M.D., Ph.D.
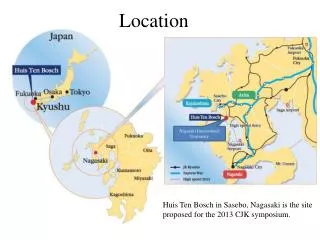
2011/9/9 4 Chronic forms of Pulmonary Aspergillosis family case, Sasebo, JAPAN 54 years old, male, SON 82 years old, male, father slowly progressive inflammatory pulmonary syndrome due to Aspergillus spp.
2011/9/9 5 Chronic forms of Pulmonary Aspergillosis family case, Sasebo, JAPAN investigation of circumstances over 50 years old wooden house humid and old
Systemic Mycosis in Japan from Autopsy Data 6 Total number of Mycosis Candidiasis Aspergillosis Cryptococcosis Mucor 5 4 3 2 1 0 FLCZ 1989 F-FLCZ 2004 MCZ 1980 ITCZ 1993 VRCZ 2005 5-FC 1979 MCFG 2002 AMPH-B 1962 L-AMB 2006 (%) ? Frequency (%) 1960 1970 1980 1990 2000 2007 Year Kume et al. Med Mycol J 52: 117-127, 2011
Proposed classification and pathogenesis of chronic pulmonary aspergillosis Preexisting pulmonary defect, with cavity Aspergillus exposure Colonization of pulmonary cavity Generalized immuno-compromised state (e.g. diabetes, AIDS, alcoholism) Subtle generalized or pulmonary defense defect Immune dysregulation No local generalized defect Nodular or consolidation, w/ or w/o cavitations: subacute invasive pulmonary aspergillosis (subacute IPA) or chronic necrotizing pulmonary aspergillosis (CNPA) Multiple cavities w/ surrounding inflamation ±aspergilloma: chronic cavitary pulmonary aspergillosis (CCPA) or complex aspergilloma Resolution of infection or asymptomatic, stable single aspergilloma: simple aspergilloma normal/weak fibrosis response strong fibrosis response continuing cavity formations and local inflamation Extensive pluero/pulmonary fibrosis: chronic fibrosing pulmonary aspergillosis (CFPA) Denning et al: Clin Infect Dis 37 Suppl 3: S265-80, 2003
Reported TB casesNew and relapse cases (per 100 000 population) 60 50 France Germany 40 Italy Japan 30 Netherlands Portugal Spain 20 Sweden United Kingdom of Great 10 Britain and Northern Ireland United States of America 0 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 WHO, Communicable Diseases Report
CPA case [case]65 Y, Male [CC] hemosputum, cough [PH] n.p. [PI] 1998:right upper lobectomy (Tbc) 2005~:cough, hemosputum 2006~: hemosputum increased chest CT:fungus ball like shadows in right lower lung. Platelia EIA: positive, Aspergillus Ab: positive β-D-gulucan 35.0pg/ml admission for further treatment [PE] Height 161cm, Weight 44.3kg, BMI 17.1, Body temp. 36.8℃, pulse 68/min, regular rhythm
8700 6700 5700 5300 6500 8000 7500 7500 1.65 5.70 0.19 0.20 0.93 1.46 3.24 0.72 39.5 117.8 90.9 68.2 47.4 25.9 28.9 0.65 0.976 0.985 1.025 0.441 0.461 0.591 0.517 CPA caseITCZ oral solution treatment 2/16 2/22 3/19 10/4 10/11 6 months BIPM 0.6g/day BIPM 0.6g/day MCFG 150mg/day VRCZ 200mg/day ITCZ 400mg/day ITCZ 200mg/day BALF: A. fumigatus A. niger A. versicolor A. terreus BALF: A. fumigatus sputum:A. terreus 37℃ hemosputum WBC(/μl) CRP(mg/dl) β-D-glucan(pg/ml) Aspergillus antigen (EIA)
12 • Evidence of CPA treatment
CPA treatment • IDSA GL NO RCT existed !! P.O. first and I.V. is optional Clin Infect Dis 2008; 46:327-360
World First RCT in CPA treatment Kohno, Izumikawa et al: J Infect, 2010
New Evidence of CPA treatmentOverall efficacy MCFG v.s. VRCZ 15 (%) P=0.543* 100 60.0% (30/50) 53.2% (25/47) efficacy 50 0 MCFG VRCZ Kohno, Izumikawa et al: J Infect, 2010
New Evidence of CPA treatment Frequency of side effect MCFG v.s. VRCZ 16 P=0.0004* (%) 61.1% (33/54) 70 60 50 frequency 40 26.4% (14/53) 30 20 10 0 MCFG VRCZ Kohno, Izumikawa et al: J Infect, 2010
New Evidence of CPA treatment Frequency of side effect MCFG v.s. VRCZ Visual disturbance & hepatic dysfunction 17 70 70 70 60 60 60 50 50 50 40 40 40 30 30 30 20 20 20 10 10 10 0 0 0 P=0.012* P<0.0001* (%) (%) (%) P=0.025* 50.0% (27/54) frequency frequency frequency 35.2% (19/54) 29.6% (16/54) 26.4% (14/53) 15.1% (8/53) 0.0% (0/53) MCFG VRCZ MCFG VRCZ MCFG VRCZ Adverse effects except visual related events Hepatic events Visual events Kohno, Izumikawa et al: J Infect, 2010
2011/9/9 18 Day1~5 Day-2 Day0 Inoculum(i.t.) immunosupression L-AMB inhalation ICR,♀,8weeks Another route of antifungal administration nebulized L-AMB & MCFG IPA murine model Day-2,0:Cyclophosphamide200mg/kg i.p.+CortisoneAcetate250mg/kg s.c. Day0: MF-13 conidia 1×108/ml:50μl intratracheal inoculation Day1~5: L-AMB1.2mg/ml:8ml nebulize once/day MCFG 1mg/kg/day intraperitoneal Group1: nL-AMB + MCFG Group2: nL-AMB Group3: MCFG Group4: Control and/ or MCFG i.p. Takazono, Izumikawa: AAC 53: 3508-3510, 2009
Another route of antifungal administration nebulized L-AMB & MCFG IPA murine model 2011/9/9 19 1 n L-AMB+MCFG .8 survival rate N L-AMB .6 MCFG .4 control .2 0 Time (DAYS) 0 2 4 6 8 10 12 14 16 Control MCFG (i.p.) L-AMB L-AMB+ MCFG (i.p.) Day3 pathology GMS stain×400 Takazono, Izumikawa: AAC 53: 3508-3510, 2009
Another route of antifungal administration nebulized L-AMB & MCFG IPA murine model 2011/9/9 20 AMPH-Bconcentration L-AMB inhalation conc. Lung (mg/kg) serum (μg/ml) control 0.1 <0.02 L-AMB 1.2mg/ml 35.5±4.2 0.02 L-AMB 2.6mg/ml 73.2±15.8 0.06 L-AMB 4.0mg/ml 94.2±20.2 0.06 Takazono, Izumikawa: AAC 53: 3508-3510, 2009
250 6 5 200 4 150 3 100 2 50 1 0 0 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 ITCZ resistant A. fumigatus Nijmegen, Netherland number % PLoS Med. 2008 November; 5(11): e219
Multi-azole ITCZ & POSA VRCZ ITCZ Susceptible AzoleresistantA. fumigatus Manchester, U.K. 100 % 20 90 80 70 5 14 60 Number of patient cases 17 50 7 5 3 40 0 0 30 5 20 7 0 0 10 0 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 Year Bueid et al. JAC 65: 2116-2118, 2010
Mechanism of action azole antifungals Ergosterol Toxic sterol Azoles Ergosterol Ergosterol P450 Erg3 P450 Erg3 14DM 14DM Toxic sterol Erg3 ー Triazole + Triazole Cowen LE. Eukaryotic Cell 2008 7:747-764
Mechanism of resistance azole antifungals Traizoles Triazoles Ergosterol Ergosterol Erg 3 Erg 3 P450 14DM P450 14DM Alternate sterol Triazoles Ergosterol P450 14DM Erg 3 Mutation Toxic sterol Erg 3 Alternation of synthesis Mutation of Erg 3 Overexpression of Efflux pumps Alternation, mutation and over expression of P45014DM Cowen LE. Eukaryotic Cell 2008 7:747-764
TR TR G54 Promoter G138 ITCZ resistance POSA resistance Multi-azole resistance Multi-azole resistance Membrane-anchoring region Mechanism of azoleresistant A. fumigatusCyp51Amutation hot spot, Netherland & U.K. Multi-azole resistance (%) L98H M220 G448 F-helix G-helix Cyp51A Membrane-anchoring region Verweij PE, et al. Lancet Infect Dis 9: 789-795, 2009
Drug susceptibility of Aspergillus fumigatus Nagasaki University Hospital Clinical Isolates (196 strains) Strains: Clinical isolated A. fumigatus between 1994 and 2010 Method of identification: microscopic morphology ability to grow at 48˚C molecular confirmation (sequence of ITS and D1/D2) Drug susceptibility test: CLSI M38 A-2 Tested antifungals: FLCZ, ITCZ, VRCZ, POSA, MCFG, AMPH-B Molecular epidemiology STR/microsatellite analysis
Drug susceptibility of Aspergillus fumigatus Nagasaki University Hospital Clinical Isolates (196 strains) frequency of non-WT isolates Itraconazole ≧2 μg/ml (14/196) 7.1 % Voriconazole ≧2 μg/ml (8/196) 4.1% Posaconazole ≧1 μg/ml (5/196) 2.6 %
Drug susceptibility of Aspergillus fumigatus Nagasaki University Hospital Clinical Isolates (196 strains) frequency of non-WT isolates and cross resistance POSA VRCZ ITCZ
Drug susceptibility of Aspergillus fumigatus Nagasaki University Hospital Clinical Isolates (196 strains) Comparison of positive rate of Cyp51A mutation to Europe
Drug susceptibility of Aspergillus fumigatus Nagasaki University Hospital Clinical Isolates (196 strains) Comparison Cyp51A mutation with Netherland TR TR G54 Promoter G138 ITCZ resistance POSA resistance Multi-azole resistance Multi-azole resistance Membrane-anchoring region Multi-azole resistance (%) L98H M220 G448 F-helix G-helix Cyp51A Membrane-anchoring region AAC. 2010; 54: 2425-30
Azole-resistant Aspergillus fumigatus Nagasaki University Hospital Clinical Isolates (196 strains) Correlation of ITCZ exposure amount and drug susceptibility 180000 150000 120000 Cumulative ITCZ exposure (mg) 90000 r = 0.5916 p <0.0001 60000 30000 0.25 0.125 0.5 1 8 4 2 >8 ITCZ MIC(μg/ml)
Azole-resistant A. fumigatus isolated case 59 years old, Male 2011/9/9 32 CC: fever, cough, sputum PH: surgical for pneumothorax β-D glucan Aspergillus Ag AspergillusAb Sputum culture (bacteria) Sputum culture (Tbc) Sputum culture 53.5 2.9 (+) (-) (-) pg/ml C.O.I. A. fumigatus
Azole-resistant A. fumigatus isolated case 59 years old, Male 2011/9/9 33 12 10 11 1 2 3 4 5 6 7 8 9 24.0 βD glucan 1999 ITCZ 200mg 53.5 15.7 6.9 Aspergillus Ag 2000 2.9 5.3 2.5 Sputum culture Serum ITCZ conc. 1.148 μg/ml MCFG 150mg 1st isolated ITCZ low-sensitive A. fumigatus 2.1 0.6 2001 ITCZ 400mg ITCZ 200mg 53.4 132.2 87.0 2002 5.1 6.6 9.1 4.9 2.9 1.5 VRCZ 300mg 7.2 2003 0.8 0.6 0.1 ITCZ 200mg MCFG 300mg
Azole resistant A. fumigatus isolated case 59 years old, Male 2011/9/9 34 MCFG 150mg ITCZ 200mg ITCZ 400mg 1/23 8/16 12/14 5/16 2001/10/22 2000/08/15 2000/12/14 2001/05/17 2002/01/23 VRCZ 300mg 6/4 8/25 2003/04/14 2002/08/27 2011/08/29 2002/02/27 2002/05/22
Azole-resistant A. fumigatus isolated case 59 years old, Male, summary of isolated strains and cases 2011/9/9 35
SUMMARY CPA treatment and drug resistance Treatment →New evidence become available by first RCT →Development of newer treatment is required Azole-resistance →It is few in Japan →Cyp51A mutation is common in drug resistant strains →Resistant may be acquired by exposure of azole
2014/9/11 37 Advertisement The 86th Japanese Society of Infectious Diseases Annual meeting 2012, Nagasaki, JAPAN
Acknowledgement • Nagasaki University • Shigeru Kohno • Takayoshi Tashiro • Katsunori Yanagihara • Yoshihiro Yamamoto • Hiroshi Kakeya • Taiga Miyazaki • Yoshifumi Imamura • Shigeki Nakamura • Takahiro Takazono • Masato Tashiro • Katsuji Hirano • National Institutes of Infectious Diseases • Yoshitsugu Miyazaki • Hideaki Ohno