Download
1 / 9
100 likes | 240 Views
ASCOT and Steno-2: Aggressive risk reduction benefits two different patient populations. Steno-2. ASCOT-LLA. Steno-2: Diabetes + microalbuminuria Intensive target-driven reduction of BP, total-C, TG, A1C vs usual care 7.8 years ASCOT-LLA:

E N D
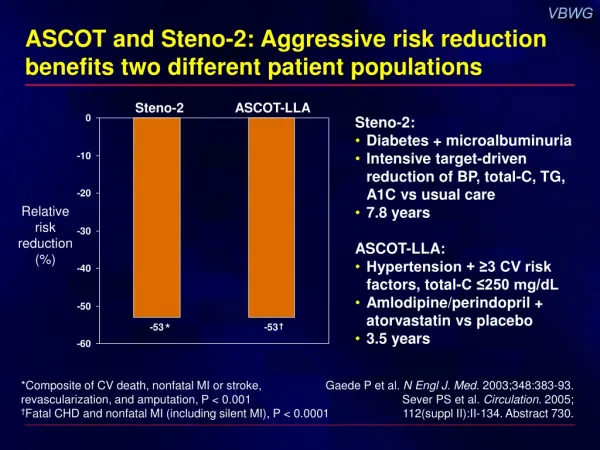
ASCOT and Steno-2: Aggressive risk reduction benefits two different patient populations Steno-2 ASCOT-LLA • Steno-2: • Diabetes + microalbuminuria • Intensive target-driven reduction of BP, total-C, TG, A1C vs usual care • 7.8 years • ASCOT-LLA: • Hypertension + ≥3 CV risk factors, total-C ≤250 mg/dL • Amlodipine/perindopril + atorvastatin vs placebo • 3.5 years Relative risk reduction (%) * † *Composite of CV death, nonfatal MI or stroke, revascularization, and amputation, P < 0.001 †Fatal CHD and nonfatal MI (including silent MI), P < 0.0001 Gaede P et al. N Engl J. Med. 2003;348:383-93. Sever PS et al. Circulation. 2005;112(suppl II):II-134. Abstract 730.
ASCOT: Patients had hypertension and ≥3 other risk factors, fitting a common clinical profile Hypertension Aged ≥55 years Male Microalbuminuria/proteinuria Smoker Family history of CHD Plasma total-C:HDL-C ≥6 Type 2 diabetes Certain ECG abnormalities LVH Prior cerebrovascular events Peripheral vascular disease 0 10 20 30 40 50 60 70 80 90 100 Patients with risk factor (%) Sever PS et al. J Hypertens. 2001;19:1139-47.Sever PS et al. Lancet. 2003;361:1149-58. LVH = left ventricular hypertrophy
ASCOT-BPLA: Reduction in primary outcome (nonfatal MI and fatal CHD) 10 8 RRR = 10% HR = 0.90 (95% CI, 0.79–1.02) P = 0.1052 6 Proportionof events (%) 4 Atenolol-based regimen* 2 Amlodipine-based regimen† 0 0 1 2 3 4 5 6 Time since randomization (years) *Atenolol 50–100 mg ± bendroflumethiazide 1.25–2.5 mg †Amlodipine 5–10 mg ± perindopril 4–8 mg Dahlöf B et al. Lancet. 2005;366:895-906.
ASCOT: Risk reductions with the amlodipine/perindopril regimen Rate/1000 patient-years Amlodipine-based*(n = 9639) Atenolol-based† (n = 9618) <0.05 <0.01 <0.0001 <0.05 0.001 <0.001 NS <0.0001 <0.05 Secondary endpoints Nonfatal MI (excluding silent) 7.4 8.5 + fatal CHD Total coronary endpoint 14.6 16.8 Total CV events and procedures 27.4 32.8 All-cause mortality 13.9 15.5 CV mortality 4.9 6.5 Fatal/nonfatal stroke 6.2 8.1 Fatal/nonfatal HF 2.5 3.0 Tertiary endpoints Development of diabetes 11.0 15.9 Development of renal impairment 7.7 9.1 Amlodipine-based better Atenolol-based better P 0.50 0.75 1.00 1.50 2.00 Unadjusted hazard ratio *Amlodipine 5–10 mg ± perindopril 4–8 mg †Atenolol 50–100 mg ± bendroflumethiazide 1.25–2.5 mg Dahlöf B et al. Lancet. 2005;366:895-906.
CAFE asked whether newer vs older BP treatments have differing effects on central aortic BP N = 2199 5 UK ASCOT centers n = 126Excluded: HR irregularity Poor waveforms N = 2073Evaluable for tonometry n = 1042Amlodipine ± perindopril* n = 1031Atenolol ± bendroflumethiazide† n = 1042 Intent-to-treatn = 1038 Complete information n = 1031 Intent-to-treatn = 1030 Complete information *Newer antihypertensive regimen †Older antihypertensive regimen CAFE Investigators. Circulation. 2006;113:1213-25.
CAFE: Central aortic pressure is lower with the amlodipine/perindopril regimen 140 Brachial SBP 135 130 Central aortic SBP mm Hg 125 120 115 0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 5.5 6 Time (years) Amlodipine ± perindoprilAtenolol ± bendroflumethiazide CAFE Investigators. Circulation. 2006;113:1213-25.
CAFE: Lesser ability of β-blockers to reduce augmentation wave P < 0.0001 Atenolol ± bendroflumethiazide Amlodipine ± perindopril CAFE Investigators. Circulation. 2006;113:1213-25.
ASCOT: Lipid lowering is beneficial regardless of baseline cholesterol level Sever PS et al. Lancet. 2003;361:1149-58.
P = 0.015 ASCOT: Greater gain with statin + CCB/ACE inhibitor vs statin + β-blocker/diuretic Fatal CHD and nonfatal MI NS P < 0.0001 NS 10 9.8 9 9 8 7 7.5 Events/1000patient-years 6 5 4 3 4.6 2 - Atorvastatin (+ placebo) 1 0 + Atorvastatin (10 mg) P (interaction between lipid and BP lowering) = 0.025 Atenolol* † Amlodipine Sever PS et al. Circulation. 2005;112(suppl II):II-134. Abstract 730. Sever PS et al. AHA Scientific Sessions. Nov 2005. *Atenolol ± bendroflumethiazide†Amlodipine ± perindopril















