Corticosteroids: Functions, Mechanism, and Applications
Learn about corticosteroids, including cortisol and aldosterone, their pharmacokinetics, mechanism of action, preparations, therapeutic uses, and precautions. Discover how these hormones regulate various physiological processes in the body.

Corticosteroids: Functions, Mechanism, and Applications
E N D
Presentation Transcript
The adrenal cortex secretes a number of steroid hormones into circulation: • Glucocorticoids: cortisol (hydrocortisone). • Mineralocorticoids: aldosterone. • Sex hormones I. Cortisol • The major glucocorticoid in humans. • controlled by ACTH secreted from the anterior pituitary. • circadian rhythm peaks in early morning & troughs at midnight. • 95% of Cortisol circulates in blood bound to globulin; Corticosteroid binding globulin (CBG).
II. Aldosterone • Most important mineralocorticoid (inhibits Na+ excretion & stimulates K+ & H+ excretion) with minimal glucocorticoid activity. • Very important in regulating blood volume & pressure. • Control of Aldosterone Secretion 1. Renin-angiotensin system activation by hypovolemia & hyponatremia (most important). 2. Hyperkalemia.
Pharmacokinetics : • cortisol is bound to corticosteroid binding globulin [CBG]. • CBG is increased by oestrogen, decreased in cases of liver cirrhosis and nephrosisof kidney, • t 1/2 is 90-110 min, • Metabolisedin the liver, • Excreted by kidneys as water soluable reduced conjuagates, about 10% is excreted as 17 - ketosteroids.
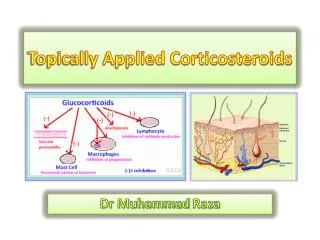
Mechanism of Action of Corticosteroids • They enter cells where they combine with steroid receptors in the cytoplasm forming a macro molecular complex which enters the nucleus where it interacts with chromosomal constituents and alters gene expression effects on organs and tissues.
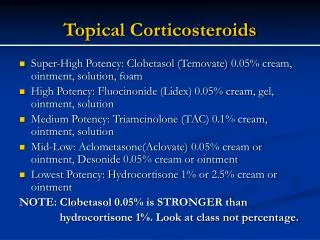
Preparations of Corticosteroids A. Preparations with Primarily Glucocorticoid Activity I. Cortisol (hydrocortisone) • Disadvantages of Cortisol 1. Mineralocorticoid activity. 2. Short duration: (t½ dramatically in liver insufficiency). 3. Poorly absorbed through normal skin (but readily absorbed through inflamed skin & mucus membrane). II. Synthetic Preparations Prednisone - prednisolone – dexamethazone. Advantages over Cortisol 1. Mineralocorticoid activity is less with prednisolone & absent with dexamethazone. 2. Longer duration of action. 3. More absorption through skin.
B. Preparations for Bronchial Asthma • Beclomethazone, budesonide, fluticasone inhalation • Advantages in Asthma 1. Readily penetrate airway. 2. Very short half lives after entering the blood (if swallowed while being inhaled) due to extensive 1st pass metabolism so that systemic effects and toxicity are greatly reduced.
Therapeutic Uses I. Adrenal Disorders A. Acute Adrenal Insufficiency (Addisonian Crisis) 1. Saline & 5% glucose maintain fluid & salt balance & blood sugar. 2. IV hydrocortisone hemisuccinate. 3. Fluodrocortisone is started when total cortisol dose is to 50 mg/d. 4. Treat precipitating factors, e.g. antibiotics for infection. B. Chronic Adrenal Insufficiency (Addison’s disease) 1. Oral hydrocortisone: dose is during stress or surgery. 2. Fluodrocortisone (orally): maintains Na+ balance & BP.
II. Nonadrenal Disorders A. Anti-allergic • 1. Bronchial asthma. 2. Allergic conditions: skin, eye, GIT. B. Immunosuppressants in: 1. Autoimmune diseases: systemic lupus - rheumatoid arthritis. 2. Organ transplantation, skin grafts. III. Other Uses 1. Cerebral edema: VD - exudation of fluids. 2. leukemia - lymphomas: lymphocytes. 3. Antistress in: bleeding - trauma - septic & anaphylactic shock ( VC effect of CA - glucose level, providing energy to counteract stress). 4. Hypercalcemia:vit. D activation in liver Ca2+ absorption). 5- Respiratory distress lung syndrome (stimulatinof lung maturation in the fetus by stimulation of surfactant production
Precautions of use of glucocorticoids: I-Avoid adrenocortical suppression by using smallest doses, alternate day schedule and gradual withdrawal. 2- The dose should increased during periods of stress in chronic therapy. 3- Diet should contain low Na+, high K+, high Ca++ and high proteins. 4- regular examination of blood pressure, blood glucose and body weight. 5-X ray spine every 6 months to detect osteoporosis. 6- anabolic steroid may be given to counteract catabolic effects. 7 - Never stop therapy suddenly to avoid acute adrenocortical insufficiency
Mineralocorticoids 1- Aldosterone: 2- Deoxycorticosterone (DOC( it is potent mineralocorticoid with no glucocorticoid action used in hypoadrenal states by IM injection or as DOCA pellet sc. 3-Fluodrocortisone • Synthetic prep. with potent mineralocorticoid & glucocorticoid activity. • used for replacement therapy in hypoadrenal states, e.g. after adrenalectomy.