CUtLASS TRIAL
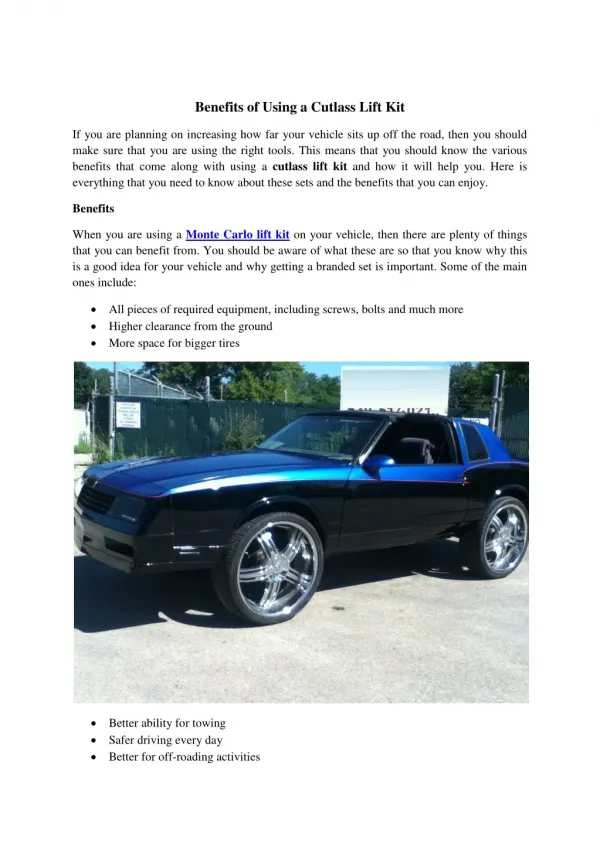
CUtLASS TRIAL. Ron Beasley, PharmD Candidate Preceptor: Soheyla M ahdavian, PharmD. CUtLASS TRIAL. C ost U tility of t he L atest A ntipsychotic Drugs in S chizophrenia S tudy Tested at Fourteen community psychiatric services in the English National Health Service .

CUtLASS TRIAL
E N D
Presentation Transcript
CUtLASS TRIAL Ron Beasley, PharmD Candidate Preceptor: SoheylaMahdavian, PharmD
CUtLASSTRIAL • Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study • Tested at Fourteen community psychiatric services in the English National Health Service. • Published in Archives of General Psychiatry in 2006
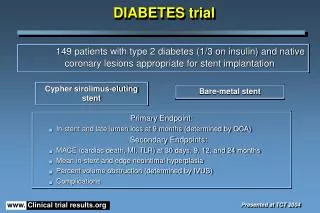
Objectives • To test the hypothesis that in people with schizophrenia SGAs improve quality of life across 1 year compared with FGAs. • Multisite, randomized controlled trial of antipsychotic drug classes, with • Blind assessments at 12, 26, and 56 weeks using intention-to-treat analysis.
Methods • 227 people aged 18 to 65 years with DSM-IV schizophrenia and related disorders assessed for medication review because of inadequate response or adverse effects. • Following randomization, the referring psychiatrists would choose a medication from the assigned class to administer for up to 1 year's duration.
Methods Cont. • The FGAs were • Chlorpromazine hydrochloride, • Flupenthixol * • Haloperidol • Loxapine • Methotrimeprazine* • Sulpiride* • Trifluoperazine hydrochloride • Zuclopenthixol* • Depot Preperations • Fluphenazinedecanoate, • Flupentixoldecanoate* • Haloperidol decanoate • Pipothiazinepalmitate * • Zuclopenthixoldecanoate * *Not in the USA
Methods Cont. • SGAs were • Risperidone • Olanzapine • Amisulpride* • Zotepine* • Quetiapine *Not in the USA
Criteria Inclusion Exclusion Substance misuse or a medical disorder considered clinically to be the major cause of positive psychotic symptoms and a history of neuroleptic malignant syndrome. • DSM-IV schizophrenia, schizoaffective disorder, or delusional disorder • Age 18 to 65 years • At least 1 month since the first onset of positive psychotic symptoms • Psychiatrist electing to change the current FGA or SGA treatment because of inadequate clinical response or in- tolerance.
Outcome Measurements • The primary outcome measure was total score on the Quality of Life Scale (QLS), assessed blindly at baseline and at Weeks 12, 26, and 52 of the study. • Secondary outcome measures included: • Positive and Negative Syndrome Scale (PANSS) • Calgary Depression Scale • Various scales looking at adverse medication effects • Participant satisfaction
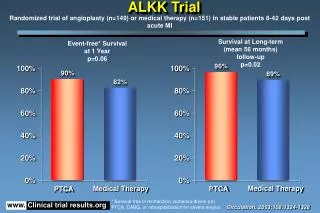
Results • SGAs did not show superiority in improvement in the QLS. In fact, there was a numerical trend toward greater improvement with the FGA cohort. • Healthcare costs were similar in both groups with psychiatric inpatient hospitalization responsible for the majority of the expense. • Although SGAs were more expensive than FGAs, total antipsychotic medication cost was a relatively small proportion of total expenses (2.1% and 3.8% for FGAs and SGAs, respectively).
Results cont. • There was no measurable difference between the 2 cohorts in: • Positive or negative symptoms • Depressive symptoms • Adverse effects
Critique (Pros) • It is consistent with several other recent studies showing minimal to no clinical or cost-savings advantage of SGAs over FGAs • It is a practical, blinded, well-designed trial that contains discussion about why the original premise (SGA superior to FGA) could not be proven • Effect size, sample size, statistical power, utility of the QLSall were assed for bias
Critique (Cons) • This study fails to answer key questions: • Are second-generation antipsychotic medications overrated? • Do SGA’s really provide patients with an advantage over first-generation antipsychotics? • Limited sample size and statistical power • Psychiatrists may have been less ready to change from SGAs compared with FGAs in treating the patients skewing results.
References • 1. Voruganti L, Cortese L, Oyewumi L, Cernovsky Z, Awad A. Comparative evalu- ation of conventional and novel antipsychotic drugs with reference to their sub- jective tolerability, side-effect profile and impact on quality of life. Schizophr Res. 2000;43:135-145. • 2. National Collaborating Centre for Mental Health. Guidance on the Use of Newer (Atypical) Antipsychotic Drugs for the Treatment of Schizophrenia. London, En- gland: National Institute for Clinical Excellence; 2002. • 3. Davis JM, Chen N, Glick ID. A meta-analysis of the efficacy of second- generation antipsychotics. Arch Gen Psychiatry. 2003;60:553-564.