Download
1 / 56
560 likes | 929 Views
Antimicrobial drugs in Respiratory Infection. Huifang Tang Department of pharmacology Zhejiang University, school of medicine tanghuifang@zju.edu.cn Research building C422 2012-3. Introduction. The key disorders of respiratory system:

E N D
Antimicrobial drugs in Respiratory Infection Huifang Tang Department of pharmacology Zhejiang University, school of medicine tanghuifang@zju.edu.cn Research building C422 2012-3
Introduction The key disorders of respiratory system: 1. Disorders of the upper respiratory tract: rhinitis(鼻炎), tonsillitis(扁桃体炎), angina(咽峡炎), laryngitis(喉炎), cold(感冒), etc. ; 2. Bronchitis(支气管炎), Pneumonia(肺炎); 3. Chronic obstructive pulmonary disease (COPD, 慢性阻塞性肺疾病, 慢阻肺); 4. Asthma(支气管哮喘, 哮喘); 5. Neoplasma: nasopharyngeal carcinoma (鼻烟癌), lung carcinoma(肺癌), etc. 6. Pulmonary tuberculosis (肺结核, PTB)
anti-microbial agents Part1. -Lactam antibiotics Part 2. Aminoglycosides (氨基糖苷类) & polymyxins(多黏菌素类) Part 3. Macrolides (大环内酯类), lincomycins (林可霉素类), and vancomycins (万古霉素) Part 4. Tetracyclines(四环素类)& chloramphenicol(氯霉素) Part 5. Synthetic antimicrobial agents(人工合成抗菌药) Part 6. Antifungal agents Part 7. Antiviral agents Part 8. Antituberculous drugs Part 9. The drugs treated parasitic infections
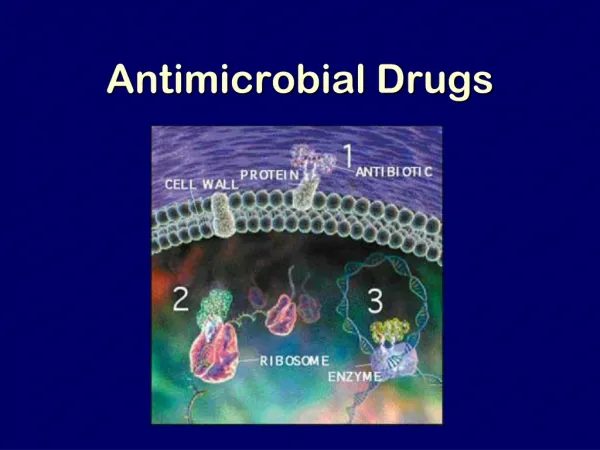
Classification and mechanism of action ① ④ ⑤ ③ ②
Contents • -Lactam Antibiotics(内酰胺类) • Macrolides (大环内酯类) • Quinolones(喹诺酮类) • Tetracyclines(四环素类) • Antituberculous drugs(抗结核药)
Classification of-Lactam Antibiotics Ⅰ. Penicillins(青霉素类) Ⅱ. Cepharosporins(头孢菌素类) Ⅲ. Other -lactam antibiotics: 1. Cephamycins(头霉素类) 2. Carbapenems(碳青霉烯类) 3. Monobectams(单环类) 4. Oxacephalosporins(氧头孢烯类) Ⅳ. -lactamase inhibitors(内酰胺酶抑制剂)
I. Penicillins 1. Classification of Penicillins: (1)Nature penicillins: Penicillin G(苄青霉素, 简称青霉素) (2)Penicillinase-resistant penicillins: Oxacillin(苯唑西林) (3)Broad-spectrum penicillins: Amoxicillin(阿莫西林) (4)Anti-pseudomonas penicillins: Ticarcillin(替卡西林) (5)Anti-G- bacilli penicillins: Mecillinam(美西林)
Penicillins Mechanism of action: (1)Inhibiting transpeptidase(转肽酶, PBP, 青霉素结合蛋白), and inhibiting the synthesis of bacterial cell walls. (2)Activation of cell-wall autolytic enzyme(自溶酶).
Semi-syntheticPenicillins: 1. Penicillins by oral administration(耐酸青霉素): Phenoxymethylpenicillin (苯氧甲基青霉素, Penicillin V) It is resistant to gastric acid, and be well absorbed(60%) when it is given on an empty stomach. Its half-life(t½) is longer than that of penicillin G. A satisfactory substitute forPenicillin Gto treat tonsilitis(扁桃体炎), or Pharyngitis(咽炎), etc.
SemisyntheticPenicillins 2. The penicillinase-resistant penicillins(耐酶青霉素): • Oxacillin(苯唑西林), • Cloxacillin(氯唑西林), • Dicloxacillin(双氯西林) • It is stable in an acidic medium, can be administrated by po, or im, iv ; and it is resistant to cleavage by penicillinase. • It is used for treatment of penicillin G-resistance staphylococcal infection.
SemisyntheticPenicillins 3. Broad spectrum penicillins(广谱青霉素): Amipicillin(氨苄西林), Piperacillin(哌拉西林), etc. They have similar antibacterial activity and a broader spectrum. All can be destroyed by -lactamase.
SemisyntheticPenicillins Broad spectrum penicillins (1)Ampicillin(氨苄西林), Amoxicillin(阿莫西林) Pseudomonasaeruginosa(铜绿假单孢菌 ——绿脓杆菌)-resistance. Clinical Uses: Upper respiratory infections; Urinary tract infections; Meningitis; Salmonella infections.
SemisyntheticPenicillins Broad spectrum Penicillins (2)Piperacillin(哌拉西林),Mezlocillin(美洛西林) They have the broadest antibacterial spectrum, and the most activity of the penicillins, with activity against Pseudo-monas aeruginosa, etc. Clinical Uses: For the treatment of the patients with severeinfectioncausedbyG-bacteria, us-uallyincombinationwithaminoglycoside (氨基苷类).
4.Anti-pseudomonas penicillins Carbenicillin(羧苄西林) Ticarcillin(替卡西林) With activity against Pseudomonas aeruginosa and some Proteus(变形杆菌).
SemisyntheticPenicillins 5. Anti-G- bacilli penicillins: • Mecillinam(美西林), • Temocillin(替莫西林) • They are bacteriostatic drugs, and havenarrowantibacterialspectrum, with activity against some G- bacilli.
II. Cepharosporins • 1. First generation: • Cefazolin(头孢唑林), Cefradine(头孢拉定), Cefalexin(头孢氨苄), etc. • (1)more active than second and third genera-tion against certain G+ microoganisms; • (2)more impervious than second and thirdge-neration to attack by staphyloccal -lactamase; • (3)less active than second and thirdgenera-tion against certain G- microoganisms; • (4)non-stable to G- bacilli -lactamase; • (5)more activity against certain Pseudomonas (铜绿假单孢菌), anaerobes(厌氧菌), etc; • (6)certain kinds have kidney toxicity.
Cepharosporins 2. Second generation: Cefuroxime(头孢呋辛), Cefamandole(头孢孟多), Cefaclor(头孢克洛), etc. (1)more active than first generation against certain G- bacilli and more impervious than first generation G- bacilli -lactamase; (2)somewhat less active than first generation against G+coccibutmorethan thirdgeneration; (3)activeagainstanaerobes(厌氧菌); (4)lack activity against Pseudomonas; (5)less toxic than first generation to kidney.
Cepharosporins 3. Third generation: Ceftazidime(头孢他啶), Ceftriaxone(头孢曲松), etc. (1)far more active than first and second gene-ration against G- bacilli; (2)be highly resistant to -lactamase produced by G- bacilli; (3)with the extended spectrum against anae-robes and Pseudomonas; (4)well absorbed, penetration into tissue, blo-od and body cavity as well in sufficient concen-tration; (5)less active than first and secondgeneration against G+ cocci; (6)less toxic to kidney.
Cepharosporins 4. Fourth generation: Cefepime(头孢匹肟), Cefpirome(头孢匹罗), etc. (1)resistant to type 1 -lactamase; (2)more active than third generation against Enterbacter(耐肠杆菌); (3)less active than third generation against Pseudomonas.
Ⅲ. Other-lactamantibiotics 1. Cephamycins(头霉素类): Cefoxitin (头孢西丁) It has the similar antibacterial activity and spectrum to the second generation cepharosporins, also can be used forthe treatment of anaerobic infections.
Other-lactamantibiotics • 2. Carbapenems(碳青霉烯类): • Imipenem(亚胺培南) • Imipenem is markered in combination with cilastatin(西司他丁)——Tienam(泰能), a drug that inhibits the degradation of imipenem by a renal tubular dipeptidase. • It has the broadest antibacterial spec-trumandthemostactivityofalltheanti-biotic.
Other-lactamantibiotics 3. Monobectams(单环类): Aztreonam(氨曲南) Carumonam(卡芦莫南) For the treatment of aerobic G+ bacilli infections. Narrow-spectrum antibiotic.
Other -lactam antibiotics 4. Oxacephalosporins(氧头孢烯类) Latamoxef(拉氧头孢) Flomoxef(氟氧头孢) Broad-spectrum antibiotic(anaerobic infections).
Ⅳ. -lactamase inhibitors(-内酰胺酶抑制剂) • Clavulanic acid(克拉维酸) • Sulbactam(舒巴坦) • Tazobactam(三唑巴坦) • Binding to -lactamases and inactivate them, thus preventing the destruction of -lactam antibiotics which are substrates for -lactamases.
Macrolides History of Macrolides 1952 Erythromycin(红霉素) 1970s Acetylspiramycin(乙酰螺旋霉素) Medecamycin(麦迪霉素) josamycin(交沙霉素) 1980s Clarithromycin (克拉霉素) Roxithromycin(罗红霉素) Azithromycin(阿奇霉素)
14碳环大环内酯类: 红霉素(erythromycin) 克拉霉素(clarithromycin) 罗红霉素(roxithromycin) 15碳环大环内酯类: 阿奇霉素 (azithromycin) 16碳环大环内酯类: 吉他霉素(kitasamycin) 交沙霉素(josamycin) 乙酰螺旋霉素 (acetylspiramycin) 麦迪霉素(medecamycin) Macrolides
Macrolides Clinical uses • As penicillin substitute in penicillin-allergic or resistant patients with infections caused by staphylococci, streptococci and pneumococci • Pertussis(百日咳),diphtheriae(白喉) • Legionella (军团菌)and mycoplasma pneumonia(肺炎支原体) • H.p infection
Macrolides Second generation macrolides antibiotics • Advantage : • Broaderspectrum, higheractivity • Orallyeffective • High blood concentration • Longer t 1/2 • Less toxicity • Mainly used in respritory tract infection
Macrolides Azithromycin (阿齐霉素,丽珠奇乐) • Has the strongest activity against mycoplasma pneumoniae(肺炎支原体) • More effective on Gram-negative bacteria • Well tolerated • T1/2 :35~48h once daily • Mainly used in respitory tract infection
Macrolides Roxithromycin (罗红霉素,严迪) • 1987 France • The highest blood concentration • F 72%~85% • Respiratory tract infection and soft tissue infection • Low adverse effects
Macrolides Clarithromycin(甲红霉素,克拉霉素) • Has the strongest activity on Gram-positive bacteria, legionella pneumophila, chlamydia pneumoniae and H.p • Good pharmacokinetic property • Low toxicity
Macrolides Third generation-- Ketolides(酮基大环内酯类) • Telithromycin (泰利霉素) • It is active in vitro against Streptococcus pyogenes, S pneumoniae, S aureus, H influenzae, Moraxella catarrhalis, mycoplasmas, Legionella, Chlamydia, H pylori, N gonorrhoeae, B fragilis, T gondii, and nontuberculosis mycobacteria. • Many macrolide-resistant strains are susceptible to ketolides because the structural modification of these compounds renders them poor substrates for efflux pump-mediated resistance and they bind to ribosomes of some bacterial species with higher affinity than macrolides.
Quinolones Classification Generation Examples 1 st (1962-1969) Nalidixic acid, 萘啶酸 2 nd (1969-1979) Pipemidic acid 吡哌酸 Cinoxacin 西诺沙星 3 rd (1980-1996) Norfloxacin 诺氟沙星 Levofloxacin 左氧氟沙星 Ciprofloxacin 环丙沙星 Ofloxacin 氧氟沙星 sparfloxacin 司帕沙星 4 th (1997-) Grepafloxacin 格帕沙星 Clinafloxacin 克林沙星 Gatifloxacin 加替沙星 Moxifloxacin 莫西沙星 Respiratory fluoroquinolone”呼吸喹诺酮”
Quinolones Quinolones Antimicrobial activity & spectrum (1) Bactericidal and have significant PAE. (2)Excellent activity against aerobic gram-negative bacteria, some agents have activity against Pesudomonas. (3) Several newer agents with improved activity against aerobic gram-positive bacteria.
Quinolones Quinolones Antimicrobial activity & spectrum (4) They also are effective against Chlamydia spp.(衣原体), Legionella pneumophila(军团菌) ,anaerobic bacteria, mycobacteria(分枝杆菌). (5) Some agents have limited activity against multiple-resistance strains. (6)Bactericidal concentration≥ bacteriostatic concentration
Quinolones Quinolones • Mechanism of actions • Topoisomerases :enzymes that control and modify the topological states of DNA in cells. • Topoisomerase I, IIIcatalyse merely the relaxation of DNA • Topoisomerase II (DNA gyrase)catalyse the supercoiling of DNA • Topoisomerase IVinvolved in the separation process of the DNA daughter chains after chromosome duplication.
Quinolones Quinolones • Mechanism of actions • The quinolone antibiotics target bacterial • DNA gyrase (gram-negative bacteria) • Topoisomerase IV (gram- positive bacteria).
Quinolones ClinicalUses Respiratory tract infections. • Have inferior activity against streptococci链球菌and should not be used as primary therapy for common upper respiratory tract infections. • Alternatives for treatment of acute exacerbation of chronic bronchitis in patients with obstructive pulmonary disease who are intolerant of or have developed resistance to first-line antibiotics. • Antibiotics with activity against Streptococcus pneumoniae, Haemophilus influenzae流感(嗜血)杆菌, and Moraxella catarrhalis卡他莫拉菌.
Tetracyclines • Clinical used tetracyclines: • Tetracycline(四环素); • Demeclocycline(地美环素, 去甲金霉素); • Metacycline(美他环素, 甲烯土霉素); • Doxycycline(多西环素, 强力霉素); • Minocycline(米诺环素, 美满霉素). (Antimicrobial activity enhanced from up to down)
Tetracyclines Antimicrobial spectrum Broad-spectrum antibiotic (1) Active against a wide range of aerobic and anaerobic gram-positive and gram-negative bacteria. (2) Effective against Rickettsia(立克次体),Coxiella burnetii(螺旋体),Mycoplasma pneumoniae(支原体),Chlamydia (衣原体), and Plasmodium (疟原虫). (3) They are not active against fungi,virus.
Tetracyclines Mechanism of action Mechanism of action: ①Chloramphenicol ②Macrolides, Clindamycin ③Tetracyclines • Inhibits binding of 30S subunit with A site • Interfering with the binding of aminoacyl-tRNA with aminoacyl site(A site)
Antituberculous Drugs Main Antituberculous Drugs: First-line agents: Isoniazid(异烟肼), 1945 Rifampin(利福平), 1965 Ethambutol(乙胺丁醇), 1959 Streptomycin(链霉素), 1944 Pyrazinamide(吡嗪酰胺), 1952 Second-line agents: Para-aminosalicylic(对氨水杨酸), Ethionamide(乙硫异烟胺) Amikacin(阿米卡星) Capreomycin(卷曲霉素) Fluoroquinolones: Ciprofloxacin(环丙沙星), Ofloxacin(氧氟沙星), etc.
Isoniazid(异烟肼, Rimifon, 雷米封,INH, Isonicotinylhydrazide) • 1. Antituberculous activity: • Bacteriostaticfor resting tubercle bacilli,andbactericidalfor actively growing tubercle bacilli. • Remarkable selectivity to tubercle bacilli (0.025 ~ 0.05 mg/ml, and to other microorganisms 500 mg/ml).
Isoniazid • 2. Mechanism of action: • Inhibiting synthesis of mycolic acids(分枝菌酸) of tubercle bacilli, the mycolic acids are essential com-ponents of mycobacterial cell walls:
Isoniazid * * NAD: nicotinamide-adenine dinucleotide (烟酰胺腺嘌呤二核苷酸, 辅酶Ⅰ)
Rifampicin(RPF, 利福平) • 1. Antibacterial activity: • Rifampicin is a broad-spectrum antimicrobial activity; • It is a bactericidal for tubercle bacilli; • It can readily penetrates most tissues and into phagocytes; • Resistance mutants occurs easily if used as a single drug.
2. Mechanism of action: • Rifampicincanbindstronglytothe bsubunit ofbacterialDNA-dependent RNA ploymerase, toinhibitbacterialRNAsynthesis selectively. • It is no effect to RNA ploymerase of mammal cell(哺乳动物的细胞).
Ethambutol Ethambutol(乙胺丁醇) • 1. Antimycobacterial actvity: • Nearly all strain of tubercle bacilli are sensitive. • Be bactericidal to intercellular and extrecellular tubercle bacilli. • Resistance to ethambutol developed very slowly in vitro. • The mechanism of action is involved in inhibition of RNA synthesis. • 2. Clinical uses: • Treatment for tuberculosis of various forms when given concurrently with isoniazid.
Streptomycin(链霉素) • Streptomycin is the first effective drug to treat tuberculosis. • It is bacteriostatic for the tuber-cle bacillus. • Resistance to streptomycin deve-loped easily when it is used alone. • Given simultaneously with other antibacterialdrugstopreventemer-gence of toxic reaction & resistance occurrence.
Pyrazinamide(吡嗪酰胺) • Presenting bactericidal activity only at a sightly acidic pH in vitro. • Well absorbed from the GI tract, and it is widely distributed through-out the body. • Tubercle bacilli develops resist-ance to pyrazinamide fairly readily, but there is no cross-resistance with other anti-mycobacterial drugs.