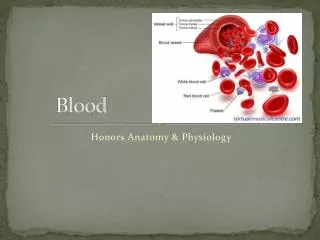
BLOOD
Blood Physiology Professor A.M.A Abdel Gader MD, PhD, FRCP (Lond., Edin), FRSH (London) Professor of Physiology , College of Medicine & The Blood Bank, King Khalid University Hospital King Saud University Riyadh. BLOOD. Lecture # 1 & 2 Topic: Red Blood Cells (RBCs).

BLOOD
E N D
Presentation Transcript
Blood PhysiologyProfessor A.M.A Abdel GaderMD, PhD, FRCP (Lond., Edin), FRSH (London)Professor of Physiology, College of Medicine &The Blood Bank, King Khalid University HospitalKing Saud UniversityRiyadh
Lecture # 1 & 2Topic: Red Blood Cells (RBCs) • Composition & functions of the Blood • Morphological Features of RBCs. • Production of RBCs • Regulation of production of RBCs • Nutritional substances need for RBC production • Haemoglobin • (Iron metabolism)
Sites of blood formation • Adults………….. Bone Marrow (Flat bones) • Children …………. Bone Marrow (Flat & long bones) • Before Birth: …. Bone Marrow Liver & spleen,lymph nodes • Fetus 1st 4 months …Yalk Sac
Monophyletic theory of cell formation Red blood cells
Hematopoiesis (17.9)
Erythropoiesis, (Formation/genesis of RBC) Growth factors (inducers): Control growth and maturation of stem cells: • Interleukin-3 • Erythropoeitin • Granulocyte stimulating factor (GSF)
Production of Erythrocytes: Erythropoiesis Figure 17.5
Erythropoiesis, (Formation/genesis of RBC) • Stages of RBC development Pluripotential haemopoietic STEM CELL Committed Stem cell Proerthroblast early, intermediate and late normoblast Reticulocytes Erythrocytes
Features of the maturation process of RBC • Reduction in size • Disappearance of the nucleus • Acquisition of haemoglobin
Lecture # 1 & 2Topic: Red Blood Cells (RBCs) • Composition & functions of the Blood • Morphological Features of RBCs. • Production of RBCs • Regulation of production of RBCs • Nutritional substances need for RBC production • Haemoglobin • (Iron metabolism)
Control of Erythropoiesis • Erythropoiesis is stimulated by erythropoietin hormone Stimulated by: • Hypoxia (low oxygen) • Anaemia • Hemorrhage • High altitude • Lung disease • Heart failure
Control of erythropoiesis Cont. • Erythropoietin • glycoprotein • 90% from kidneys 10% liver • Stimulates the growth of: earlyRBC-committed stem cells • Can be measured in plasma & urine • High level of erythropoietin • anemia • High altitude • Heart failure
Control of erythropoiesis cont. Other hormones • Androgens, Thyroid, cortisol & growth hormones are essential for red cell formation • Deficiencies of any one of these hormones results in anaemia
Erythropoitein- Mechanism of production of Hypoxia, (blood loss) • Blood O2 levels Tissue (kidney) hypoxia Production of erythropoietin plasma erythropoietin Stimulation of erythrocytes production Erythrocyte production
Lecture # 1 & 2Topic: Red Blood Cells (RBCs) • Composition & functions of the Blood • Morphological Features of RBCs. • Production of RBCs • Regulation of production of RBCs • Nutritional substances need for RBC production • Haemoglobin • (Iron metabolism)
Nutritional requirements for RBC formation • Amino acid • HemoGlobin • Iron • HemoGlobin • Deficiency small cells (microcytic anaemia )
Nutritional requirements for RBC formation cont. 3. Vitamins • Vit B12 and Folic acid • Synthesis of nucleoprotein DNA • Deficiency macrocytes megaloblastic (large) anemia • Vit C • Iron absorption
Production of Erythrocytes: Erythropoiesis Figure 17.5
Vitamin B12 & Folic acid • Important for cell division and maturation • Deficiency of Vit. B12 > Red cells are abnormally large (macrocytes) • Deficiency leads: • Macrocytic (megaloblastic) anaemia • Dietary source: meat, milk, liver, fat, green vegetables
Vitamin B12 • Absorption of VB12 needs intrinsic factor secreted by parietal cells of stomach • VB12 + intrinsic factor is absorbed in the terminal ileum • Deficiency arise from • Inadequate intake • Deficient intrinsic factors • Pernicious anaemia
Nutritional requirements for RBC formation cont. • Essential elements • Copper, Cobalt, zinc, manganese, nickel • Cobalt Erythropoietin
ANAEMIAS • Definiation • Decrease number of RBC • Decrease Hb • Symptoms: Tired, Fatigue, short of breath, (pallor, tachycardia)
Causes of anaemia 1. Blood Loss • acute accident • Chronic ulcer, worm 2. Decrease RBC production • Nutritional causes • Iron microcytic anaemia • VB12 & Folic acid megaloblastic anaemia • Bone marrow destruction by cancer, radiation, drugs Aplastic anaemia. 3. Haemolytic excessive destruction • Abnormal Hb (sickle cells) • Incompatible blood transfusion
The most common cause for a hypochromic microcytic anemia is iron deficiency. The most common nutritional deficiency is lack of dietary iron. Thus, iron deficiency anemia is common. Persons most at risk are children and women in reproductive years (from menstrual blood loss and from pregnancy).
The most common cause for a hypochromic microcytic anemia is iron deficiency. The most common nutritional deficiency is lack of dietary iron. Thus, iron deficiency anemia is common. Persons most at risk are children and women in reproductive years (from menstrual blood loss and from pregnancy)
Macrocytic anemia The RBC are almost as large as the lymphocyte. Note the hypersegmented neurotrophil. There are fewer RBCs.
The RBC's here are smaller than normal and have an increased zone of central pallor. This is indicative of a hypochromic (less hemoglobin in each RBC) microcytic (smaller size of each RBC) anemia. There is also increased anisocytosis (variation in size) and poikilocytosis (variation in shape).
Macrocytic anemia Note the hypersegmented neurotrophil and also that the RBC are almost as large as the lymphocyte. Finally, note that there are fewer RBCs.
Polycythemia • Increased number of RBC • Types: • True or absolute • Primary (polycythemia rubra vera): uncontrolled RBC production • Secondary to hypoxia: high altitude, chronic respiratory or cardiac disease • Relative • Haemoconcentration: • loss of body fluid in vomiting, diarrhea, sweating