Download
1 / 14
140 likes | 294 Views
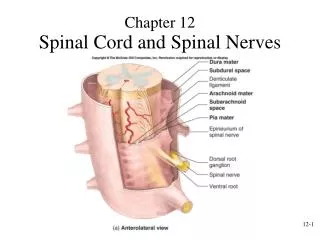
Retained Spinal Needle (stylet) Presenter: Ann McCarter Hospital: Hawk. 30-31 August Brisbane. Clinical Governance Flow Diagram. The Incident. Patient to ED for ? viral meningitis , CT brain & lumber puncture performed in ED

E N D
Retained Spinal Needle (stylet)Presenter: Ann McCarter Hospital: Hawk 30-31 August Brisbane
The Incident • Patient to ED for ? viral meningitis , CT brain & lumber puncture performed in ED • Admitted to ward, antibiotics, ID Review, ? other causes , ?TB 2nd lumber puncture D/C • 3/12 later pt to GP with ongoing back pain- GP organised CT scan • CT scan showed a needle in the spinal canal • GP contacted hospital, hospital organised pt. to return to ED, neurosurgeon consult, transferred to neurosurgical centre for r/o foreign body, identified as stylet from spinal needle
Reporting of the incident formally • Incident reported by phone call from GP to DMS, logged as a SAE . • SAE process followed as per flow for Risk Identification & Management • Key issues – time lapse between initial admission and representation
FLOW FOR RISK IDENTIFICATION AND MANAGEMENT – FLAGGING SAEs - August 2005 - Re-active Risk Identification Serious Adverse Event Patient Incident System Staff Incident System Complaint System Medico- Legal System Other Risk Identifiers An adverse event is an actual or potential occurrence outside of the norm or routines of patient care/ service delivery. A Serious Adverse Event (SAE) is where one or more patients, visitors or staff are/could be involved in an incident resulting in harm to a person(s) or property which is likely to result in significant legal, media or gov. interest. Mthly Risk Reports (RCA summaries, SAEs, System Risks) EH Exec. Qual. & Risk C’tee • Executive Member • Oversees: • documentation • notification to external agencies • as required eg VMIA, DHS • (sentinel event), coroner & others • as required eg CEO, GM, Corp. • Communications, Corp. Counsel EH Risk Register SAE Entry Within 48 hours of event Executive Member to notify hospital/program quality manager of any events falling within the following SAE definition. Event will then be added as an SAE flag on the Risk Register. SERIOUS ADVERSE EVENT – an occurrence outside the norm or routines of patient care/ service delivery that falls within the one or more of the following actual or potential outcome definitions: Patient: Major injury/death or unexpected complication to single or > than one patient; DHS Sentinel Event Staff: Major injury/death to single or > than one staff member Services: Significant cancellation of/disruption to patient care services Reputation & Image: Major threat to reputation with likelihood of significant adverse media coverage and DHS review. Financial: Event will result in major financial loss. Id’d System Risks & Actions added to Register; SAE Entry updated to System Risk RCA Flag added to SAE Entry; RCA proforma attached to Register when complete NO Notify person in charge of shift /dept /hospital co-ordinator of event immediately Are possible system issues assoc. with the SAE? Is an RCA required to explore possible system issues? Campus/Program NO YES YES Root Cause Analysis Instigate immediate harm reduction strategies UNSURE RCA Action Plan Refer for Peer/Clinical, Non-Clinical Review Dept/ Unit Head/ Hosp. Co-ordinator verbally notifies relevant Executive (eg DMS, GM) • Event details to be provided to the Quality M’ger: • What happened (including outcome) • Where it happened • When it happened • Who has been notified (internal & external) • How it will be followed up (flagged review process) Clinical stream/ program review and approval Entry closed on Risk Register Event recorded on appropriate adverse event reporting system eg Riskman (pt event), SAP (staff event) with follow-up tracked & individual & trended adverse event reports generated and reported. Clinical Council/ Corp. C’tee Facilitate learning across EH Campus/Program Quality C’tee trended adverse event reports Report
Presented to ED with? Meningitis CT and Lumbar puncture performed Further investigation required in the ward, prior to discharge- cytology and AFB LP performed Discharged home after 2/52 course of antibiotics . Inv. WNL Seen by ID Registrar in OPD. Back or leg pain not documented Provisional diagnosis of viral meningitis-? Partially treated bacterial meningitis. Commenced on IV antibiotics Visited GP with Back Pain LP done by Intern under supervision by Registrar CT showed broken needle in spinal canal Pt since informed hospital that she experienced pain shooting down the leg at the time of procedure. However not d/w operators at the time Hospital contacted patient immediately. Conveyed our regret and organized urgent neurosurgical consultation. Discharged home post removal of broken stylet. No neurological deficits reported. Transferred to Neurosurgical Centre, the same day RCA commissioned Follow up phone call to check on condition. Letter to GP Has some ongoing back pain GP contacted hospital, with findings Incident Review Process
Key findings and recommendations • Presentation of & the use of multiple needles in pack could result in mixing of stylet and needles resulting in possible shearing off of the stylet, if bent during procedure. • Lack of familiarity with needles used for the procedure could result in inadvertent use of wrong needles and/ or techniques. 3. Lack of checklist to indicate what needles are ideally suited for which situation, could result in confusion and where there is lack of experience, selection of wrong needles could result in unsuccessful lumbar puncture requiring repeat punctures.
Key findings and recommendations Incidental findings • There is a trend among ED physicians to use smaller spinal needles to avoid post dural puncture headache. Small spinal needles may have a greater risk of breaking or bending, and greater likelihood of collecting insufficient CSF. 2. Registrar’s may not do enough lumbar punctures to maintain skill levels or to provide adequate supervision to junior staff. 3. Lack of documentation when lumbar punctures are performed, specifically lack of notation regarding site of puncture, ease or difficulty of procedure, size/type of needle used, amount of CSF taken.
Key findings and recommendations Key barriers/issues and how were they overcome? Barriers – Time lapsed, not being able to identify exactly what happened . Intern concerned now working in Perth Overcome by – Working on assumptions /reproduced scenario/role play Telephone interviews
Closing the loop Outcome – • Training and Skill development for interns to become familiar with equipment and procedure prior to undertaking procedures on patients • Strategies to maintain Registrar’s skills to enable supervision of junior staff • Review available needles, their uses and standardize spinal needle packs • Develop a procedure sheet for documentation of defined information following a lumbar puncture. The procedure sheet to also incorporate a check list for selection of needles to suit the purpose of LP.
Closing the Loop • Open disclosure process? Yes, hospital part of the National Open Disclosure Pilot. Patient knew about the incident so open disclosure process was about giving feedback,the results of RCA and supporting patient. • How did you close the loop with staff? Findings on the HMO’s Website, changes in practice publicised in “Risky Business”, Topic for Grand Round, Wards & CSSD received email re changes to packs, EH Product Evaluation Review for cross campus follow-up
Open Issues What still needs to be fine-tuned or improved in regard to the above incident? • Documentation Template • Skills of Registrars • Audit of Lumber Puncture packs –planned for November 06 • Review practice in Emergency Department