Download
1 / 37
370 likes | 418 Views
Explore the role of cerebral plasticity in PresbyCor treatment for presbyopia, with insights into brain adaptation and visual accommodation. Learn about the latest advancements in refractive surgery techniques and outcomes.

E N D
The XVII All-Russian Conference Modern Technologies in Cataract and Refractive Surgery 26th–29th of October, 2016, Moscow Brain Plasticity and PresbyCor Treatment Visual Accommodation and Cerebral Adaptation
Evaluation of Cortical Plasticity following PresbyCor Dr Charles Ghenassia, M.D. France Dr Daniel-Robert Chebat Israel Charly Ruchon, Opt. France Prof. Maurice Ptito Denmark Canada Question : Is Presbyopia just a corneal or lens problem ? Does the Presbycor treatment reactivate accommodation through cerebral plasticity? What is the role of the brain?? This is the topic of our study with Dr Chebat and Prof Ptito For us, Presbylasik should not be limited to multifocality, depth field or monovision. No Financial Interest
My experience : Presbyopia surgery for 28 years I have tried different techniques, using the latest laser technology and devices • 1988 : RK L Haverbeck bifoc Kera started in place of MonovisionTMS • 1995 to 1997: Centered Presbylasik + Binoc.Vision, Multifocality(Technolas 117) • 1998 to 2003: Decentered Presbylasik (Technolas 217 C)(Coma) (ORBSCAN) • 2003 to 2005: Presbylasik guided by aberrations (Tech Z 100 Zywave ) • 2005/2015:Presbyfemtolaser guided by Asphericity + OQAS+ I TRACEY Residual Accommodation Femtoseconde + WaveLight Allegretto 2OO My own Experience • 2000/2008: Diffractive and refractive Implant surgery, Presbysmart Plus • 2007/2011 Intracor / Supracor / Presbycor WaveLight Allegreto EX 500 • 2016: SMILE mono vision, ZEISS. FMRI to study brain plasticity
I was operated 10 years ago for presbyopia. At this time we noticed an improvement in asphericity, accommodation and visual quality with OQAS Pre op RE Post op RE 10 months
Stable result at 10 years for DV and NV Without myopia or monovision Pre op RE Post op RE at 6 ½ years Question : What made Near Vision work? Depth Field and/or Accommodation, aberration compensation and brain plasticity
Between different stimuli,retinal blur is the dominant cause of accommodation
The goal of PresbyCor: To recreate the physiological principle without monovision, as in a young patient ,with compensation of lens and corneal spherical aberration during accommodation. SA Compensation during accommodation Negative Internal SA -0.16 µ - Positive Corneal SA +0.12 µ -
In Presbyopia, due to the flattening of the cornea, thereis an increase in sphericalcorneal aberration and of course a decrease in internalnegative aberration due to less flexible lens SA increase with age Antonio Guirao, Manuel Redondo, Pablo Artal: Optical aberrations of the human cornea as function of age. J. Opt. Society of America Vol.17, 10/october
If we increase negative corneal asphericity = We decrease positive corneal spherical aberration Q post op: -1,05 Q pre op: 0,05 Positive SA pre op : 1,350 Positive SA post op: 0,013
Depth Field plays a minor role in NV. The average value of depth field as reported in studies is 0.30D. Per Malecaze, the value obtained with dynamic aberrometry is 0.60 D (not enough to give an adequate NV) focal point P1 P2 retina -2.2D 45cm -2.5D 40cm -2.8D 35cm 5 cm 5 cm (B. Wang Depth of focus of the human eye, Survey of Ophtalmology, Volume 51, Issue 1)
Literature: what do we know about brain plasticity? • Laser correction of visual defects is limited by the brain’s capacity to adapt • Even when a visual defect is perfectly corrected, it is the brain that determines our visual acuity (Rosa, et al., 2013) • Studies have shown that vision can be restored even in patients that have been blind for a long time or that were born blind (Urbanski 2014, Sinha et al. 2013) • The brain can adapt beyond the critical growth period (Karmarkar et Dan 2006) • Studies in myopic patients treated by refractive surgery show changes in plasticity in their primary visual cortex (Vuori 2012)
Presbyopia: ifCorneal SA becomes more positive with age, PSF is worse, and this inhibits brain perception and thus the accommodative reflex Antonio Guirao, Manuel Redondo, Pablo Artal: Optical aberrations of the human cornea as function of age. J. Opt. Society of America Vol.17, 10/october SA+ Q=0 >0 Positive corneal spherical aberration Drawing by A. Péchereau
With PresbyCor: If we induce a hyperprolate shape that reduces positive corneal SA and retinal blur, the improved image quality (PSF) leads to an improvement in accommodation through brain plasticity Antonio Guirao, Manuel Redondo, Pablo Artal: Optical aberrations of the human cornea as function of age. J. Opt. Society of America Vol.17, 10/october 2007. SA+ Q – 0.80 Positive corneal spherical aberration Drawing by A. Péchereau
Necessary preop PresbyCor exams Pentacam Cataracte index Corneal asphéricity ITRACE Pre op criteria OQAS Simulated and Dynamic Residual Accommodation Internal & corneal aberrations Before PresbyCor, it is important to determine residual accommodation (OQAS), corneal aberrations, asphericity, and the cataract index (Miol).
The PresbyCor Software is designed to calculate the nomogram, for all presbyopic ametropias, for a target asphericity of -0.80, when using the Alcon F-cat software CORRECT VALUES TO TREAT PRE OP MEASUREMENT Target Q value myopia Target Q Value hyperopia
Advantages of the PresbyCor Treatment • One-shot treatment • takes into account : - the over- or undercorrecting shift (created by the F-Cat software) - keratometry and asphericity - residual accommodation • The post op results 1°Increase in accommodation: OQAS 2°Aberrations : I-TRACEY / change direction of lens SA 3°Contribution of Brain Plasticity ?
Study conducted on 100 patients Protocol: - Bilateral surgery without monovision Femtolaser : - flap diameter: 9.2 mm - Thickness : 110µ Wavelight Allegretto EX 500 : - asphericity : Q= -0.80 - Calculated using PresbyCor .
First Proof with OQAS: accommodation improved from 0.69 D. pre op to 2.00 D. in post op Diopters Pre-op Post-op Post-op post-op Post-op Post-op 1 month 3 months 6 months 9 months 12 months
Second proof , Itracey: compensation of Spherical Aberration as in young people The study shows a change of direction in lens SA, tied to a recovered accommodation with only an aspherical corneal treatment! Ordinate values 10-3 µ PresbyCor Pre-op Post-op Post-op Post-op Post-op Post-op 1 month 3 months 6 months 9 months 12 months
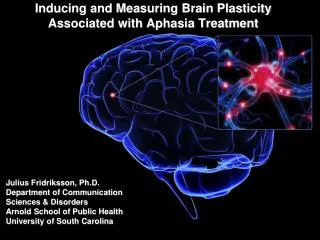
Third Proof : Ongoing fMRI Study To answer the following questions: • Is presbyopiatied to corneal or lensagingand/or a lack of brainplasticity? • Does the changing of cornealasphericitypromote the stimulation of cerebralplasticity and accommodation??
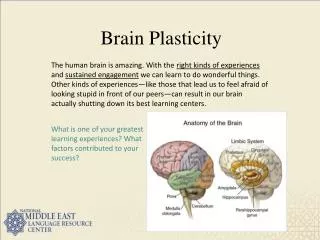
Describing Brain Plasticity Life experiencesinduce changes in brain structure and connectivity. Brain plasticityrepresentsthiscapacity to adapt.
This suggests that the brain is pliable, like plastic, and can be molded into differentforms in response to the environment including injury or abnormal genes.
Brain Plasticity and Ophthalmology • It is the interaction between the brain and the retina that determines visual performance (for review: Rosa et al., 2013; Chatard et al., 2015).
An example of the link between eye pathology and brain plasticity • Significant difference in serum BDNF concentrations between normal controls and glaucoma patients. Ghaffarieh et al., (2011) Brain-Derived Neurotrophic Factor as a Biomarker in Primary Open-Angle Glaucoma. Optometry and Vision Science
Grey matter density reductionin AMD and glaucoma • Glaucoma causes a degeneration of the LGN, visual cortex and optic nerve (Gupta et al., 2006) • Cortical grey matter density reduction in glaucoma is found in the anterior half of the medial occipital cortex (cyan). • Cortical grey matter density reduction in AMD (magenta) is found in the posterior part of the occipital cortex Boucard et al., (2013) Changes in cortical grey matter density associated with long-standing retinal visual field defects. Brain.
Increasein Grey Matter Volume of Visual Cortex after Unilateral Cataract Removal • Structural grey matter change in the visual cortex after cataract surgery. The statistical parametric map indicates relative increases in regional grey matter volume during the postoperative observation period (i.e., from day 2 to week 6–7 after s surgery). Lou et al., (2013) Postoperative increase in grey matter volume in visual cortex after unilateral cataract surgery. Acta Ophthalmologica.
Volumetric Cortical Changes following Sight Restoration in the Adult Brain • Voxel-based morphometry (VBM) analyses in KL before and after sight cataract removal. A case of sight recovery after lifelong visual impairement. Dormal et al., (2014) Tracking the evolution of crossmodal plasticity and visual functions before and after sight restoration. J Neurophysiol.
Functional Plastic Changes in Primary Visual Cortex following Refractive Surgery • Preoperative and postoperative maps of the multifocal responses for 2 anisometropic, myopic and 1 control subject. fMRI activation clusters representing the 30 stimulus regions in the left visual field. • Retinotopic map changes in the primary visual cortex Vuori et al., (2012) Refractive surgery in anisometropic adult patients induce plastic changes in primary visual cortex Acta Ophthalmologica.
Our Study (ongoing) • 30 participants: with the samevisualpathology, sameage, samepathologicalonset. • Ophtalmological Evaluation pre and post op,withseveralfollowups. • T1 and T2 Brain Scans • fMRI scans: before and after the refractivesurgery. • Scans and Diffusion Tensor Imaging (DTI). • Wecan observe the cortical changes tied to the improvement of visual performance.
T1 and T2: Cortical thickness and volumetry Voxel based morphometry (VBM) allows the visualization of volumetric changes
Visuotopia for the visual field • This technique will allow us to visualize the representation of the visual field on the cortical surface and to observe pre and post surgical changes.
Plastic Cortical Changes induced by the Accomodation Changes: fMRI while patient is reading • Before and After Refractive Surgery
Diffusion Tensor Imaging To see the strength of connections • Allows the visualization of nervous fibers that connect cortical areas. • We can visualize changes in the visual areas in the brain and test the strength of connexions.
Conclusion • There is plasticity in the adult visual cortex. • Improvement of Visual Performance after refractive surgery indicates plastic re-organization of the brain. • We can visualize plastic changes using the latest sophisticated neuroscience tools and analysis techniques.
As Glenn GOULD, the famous pianist, said: « A pianist plays the piano not with his fingers but with his mind » Our corollary : «It is not with our eyes that we see, but with our mind »
Resting State fMRI and Glaucoma Before and After Surgery • 23 participants. Areas of significant (p < 0.05) difference between Post and Pre surgery. Left MOG and right cuneus and left precentral gyrus) between Post- and Pre-PACG patients. MOG, right cuneus and left precentral gyrus. Cai et al., (2015) Network Centrality of Resting-State fMRI in Primary Angle-Closure Glaucoma Before and After Surgery. Plos One.