Download
1 / 48
480 likes | 768 Views
Clinical Scenario 1. 45 year old manHGV driver2 stone weight loss6 month history of increasing thirst and polyuriaSmokes 20 cigarettes per dayAdmits to drinking 10 units of alcohol per dayBMI 32Saw GP 2 years ago for ED tried sildenafil unsuccessfully, was advised to lose weightNo family h

E N D
1. A new patient with type 2 diabetes: What should I do? Dr Craig Parkinson
Department of Diabetes and Endocrinology
The Ipswich Hospital
12th Jan 2010
2. Clinical Scenario 1 45 year old man
HGV driver
2 stone weight loss
6 month history of increasing thirst and polyuria
Smokes 20 cigarettes per day
Admits to drinking 10 units of alcohol per day
BMI 32
Saw GP 2 years ago for ED � tried sildenafil unsuccessfully, was advised to lose weight
No family history of type 2 diabetes
Urinary analysis shows ++++ glycosuria, no ketones
Random glucose 18 mmol/l
Admission to hospital in Newcastle 5 weeks ago with abdominal pain � no further details known
3. Clinical Scenario 2 36 year old woman
Accountant
Seeks medical advice regarding pregnancy
Oligo-amenorrhoea for 3 years
BMI 36
Screening investigations reveal glucose of 9.8 mmol/l
OGTT shows 2 hour value of 12.1 mmol/l, HBA1c 8.7%
Urine analysis reveals ++ proteinuria
BP 150/88
Strong family history of type 2 diabetes � mother and brother affected
Strong family history of ischaemic heart disease (mother MI aged 50)
4. Clinical Scenario 3 40 year old woman
Teacher
Seeks medical advice regarding vaginal thrush
Treated unsuccessfully with OTC therapies
Admits to a 3 week history of tiredness, weight loss of 4 kg and thirst, polyuria and nocturia
Blurred vision
BMI 32
Screening investigations reveal glucose of 15.9 mmol/l
No family history of type 2 diabetes
5. Clinical Scenario 4 68 year old man
Retired bank manager
Routine assessment in well man clinic
Incidental finding of a fasting glucose of 17mmol/l
HBA1c 11%
Microalbuminuria positive (ACR 7)
BP 156/82 despite ramipril 10mg, amlodipine 10mg, bendroflumethazide 2.5mg and doxazosin 4mg daily
eGFR 34
Known ischaemic heart disease � MI 2 years ago, poor LV function on ECHO.
BMI 42
Has tried to lose weight using orlistat but could not tolerate this
6. Confirm the Diagnosis Consider stress hyperglycaemia if patient unwell
Diagnostic tests for diabetes (WHO criteria)
Fasting glucose of =7mmol/l
If asymptomatic confirm with second test
OGTT (must be performed correctly)
Fast from midnight
75g oral glucose in 300m of water
Baseline venous plasma glucose and at 2 hours
Diabetes confirmed if 2 hour value =11.1 mmol/l
Fasting glucose of 6-6.9 implies impaired fasting glucose
Impaired glucose tolerance
Fasting < 7mmol/l, 2 hour level >7.8 but <11.1
HBA1c > 7% makes diabetes likely (sensitivity 98% but specificity lower)
7. Confirm the Diagnosis DUK have formerly suggested that all patients with IFG have an OGTT
IFG and IGT are not interchangeable. Represent distinct abnormalities of glucose metabolism (fasting v. post prandial)
Both carry increased risk of:
progression to type 2 diabetes
Screeing?
Metformin?
Lifestyle modification should be advised
Cardiovascular risk
Assess in detail � Aspirin and Statin?
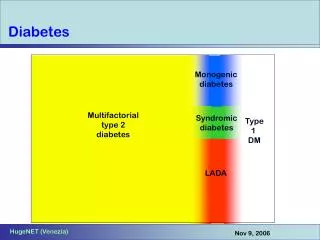
8. Consider Diagnosis Is it type 2 Diabetes?
Type 1
Usually young (<40) but may occur at any age
Prone to ketoacidosis � may be mode of presentation
Often rapid onset of profound symptoms with short history
Weight loss marked
Family history may be present but less typical
Type 1 may occur in obese individuals
9. Consider Diagnosis Type 2
Older age group
Often obese
Often asymptomatic
Symptoms may be mild to moderate and often protracted
Rapid weight loss unlikely (may hint at progressing pancreatinc malignancy � Abnormal LFTs common due to NASH)
Strong family history (100% concordance between identical twins)
Mode of presentations may be diabetic complication(s)
10. Consider Diagnosis Grey Cases
MODY
Not linked to obesity
1-2% of those with diabetes
Develops before age of 25
Strong genetic predisposition (Autosomal dominant inheritance)
11. Consider Diagnosis MODY
Six subtypes identified
HNF1a (70%) � very sensitive to sulphonylurea therapy
Glucokinase deficiency (10%) � often asymptomatic and usually no treatment required
HNF4 a - birthweight > 4kg. SU appropriate but progression to insulin therapy likely over time
HNF1� (associated with renal cysts, uterine abnormalities) � insulin usually required
Often treated with life (healthier diet and increased physical activity), some forms treatment with tablets or insulin
most types of MODY can still lead to complications glycaemic and BP control and cholesterol
LADA
Ketone prone type 2 diabetes
12. Consider Diagnosis The following characteristics suggest the possibility of MODY:
Mild to moderate hyperglycemia (7-10 mm0l/l) discovered before 30 years of age.
A first degree relative with a similar degree of diabetes.
Absence of positive antibodies or other autoimmune condition in patient and family.
Low insulin requirements (<0.5 u/kg/day) past usual honeymoon period.
Absence of obesity or other problems associated with type 2 diabetes or metabolic syndrome
Cystic kidney disease in patient or close relatives.
13. Assess Complications