Download
1 / 42
540 likes | 1.14k Views
Genetics of Lipoprotein Disorders. Jacques Genest MD Cardiovascular Genetics Laboratory McGill University Health Center. Epidemiology and Lipoprotein Metabolism Genetics of Lipoprotein Disorders Disorders of HDL; Diagnosis and Treatment.

E N D
Genetics of Lipoprotein Disorders Jacques Genest MD Cardiovascular Genetics Laboratory McGill University Health Center
Epidemiology and Lipoprotein Metabolism Genetics of Lipoprotein Disorders Disorders of HDL; Diagnosis and Treatment Human Biochemical Genetics 2008Genetics of Lipoprotein Disorders
Atherosclerosis Libby P. Inflammation and atherosclerosis. Nature 2002;420:868
Cigarette Hypertension LDL-cholesterol (apo B) HDL-cholesterol Diabetes Age Atherosclerosis Risk Factors for CAD Circulation 2000;101:111-116
Risk Factors and risk of MI Women Men Smoking Diabetes Hypertension Abd. Obesity Psychol index Fruits/Veg Exercise (-) Alcohol (-) Apo B / Apo AI Yusuf S et al. INTERHEART Lancet 2004;364:937-952
Apo B / AI Ratio (Chol/HDL-C) Yusuf S et al. INTERHEART Lancet 2004;364:937-952
Overall Western Europe Central Europe Middle East Africa South Asia China / HK SE Asia ANZ South America North America Risk of MI and apo B / AI Ratio Yusuf S et al. INTERHEART Lancet 2004;364:937-952
Genetics and CAD • Genetics of CAD are complex. • Family Hx of premature CAD increases risk > 2.0 fold • <55 for father; <65 for mother • Corrected for other RF Lloyd-Jones D et al. Lancet 2004;291:2204
Global Mortality 2020 • 1. Ischemic Heart Disease • 2. Cerebrovascular Disease • 3. COPD • 4. Diarrheal Diseases • 5. Lung Cancer • 6. Accidents • 7. Tuberculosis (without HIV) • 8. Perinatal Disorders • 9. Lower Resp Infections • 10. Suicide Lancet 1997;9061
Disability-Adjusted Life Years, 2020 • 1. Ischemic Heart Disease • 2. Unipolar Major depression • 3. Road-Traffic accidents • 4. Cerebrovascular Disease • 5. COPD • 6. Lower Resp Infections • 7. Tuberculosis • 8. War Injuries • 9. Diarrheal Diseases • 10. HIV Lancet 1997;349:1498
Within intestinal cells (and other body cells) some of the absorbed cholesterol is esterified to fatty acids, forming cholesteryl esters. (R = fatty acid chain) The enzyme that catalyzes cholesterol esterification in plasma is LCAT (Lecithin:Cholesterol Acyl Transferase) and intra-cellularly, ACAT (Acyl CoA: Cholesterol Acyl Transferase).
H O Cholesterol Cholesteryl Ester O LCAT
Triglycerides Lipoprotein Lipase
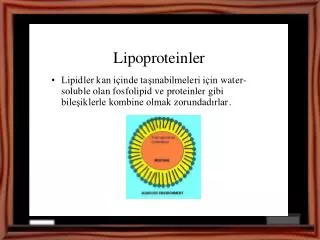
CH3 CH3-N-CH3 CH2 CH2 O O=P-O O CH2-CH-CH2 O O O=C C=O R1 R2 Phospholipids Choline Phosphate Glycerol Acyl Chains (Fatty acids)
Apolipoprotein Phospholipid Triglyceride Cholesterol Cholesteryl ester
Lipoproteins Lipoproteins differ in their contents of proteins and lipids. They are classified based on density. • Chylomicron (largest; lowest in density due to high lipid/protein ratio; highest % weight triacylglycerols) • VLDL (very low density lipoprotein; 2nd highest in triacylglycerols as % of weight) • IDL (intermediate density lipoprotein) • LDL (low density lipoprotein, highest in cholesteryl esters as % of weight) • HDL (high density lipoprotein; highest in density due to high protein/lipid ratio)
5 10 20 40 60 80 1000 0.95- VLDL 1.006- IDL CHYLOMICRON RENNANTS 1.02- Density (g/ml) LDL 1.06- HDL2 1.10- HDL3 1.20- Diameter(nm)
Lipoprotein Metabolism FFA Liver HL LPL Exogenous Pathway Chylo Remnant Chylomicron Peripheral Cells Free Cholesterol ApoA-I, A-II ApoC-I, C-II, C-III Phospholipids Free cholesterol Intestine Steroidogenic Cells HL LCAT HDL3 Nascent HDL HDL2 LDL Liver ApoA-I, A-II ApoC-I, C-II, C-III Phospholipids Free cholesterol CETP PLTP Tg Endogenous Pathway CE 3 Liver HL LPL VLDL IDL FFA
Epidemiology and Lipoprotein Metabolism Genetics of Lipoprotein Disorders Disorders of HDL; Diagnosis and Treatment Human Biochemical Genetics 2008Genetics of Lipoprotein Disorders
Case 1 • 34 yo Man • Admitted to ED with abdominal pain • Plasma lactescent • Triglycerides 154 mmol/L
Lipoprotein Lipase FFA Liver HL x LPL Exogenous Pathway Chylo Remnant Chylomicron Peripheral Cells Free Cholesterol ApoA-I, A-II ApoC-I, C-II, C-III Phospholipids Free cholesterol Intestine Steroidogenic Cells HL LCAT HDL3 Nascent HDL HDL2 LDL Liver ApoA-I, A-II ApoC-I, C-II, C-III Phospholipids Free cholesterol CETP PLTP Tg Endogenous Pathway CE 3 Liver HL LPL VLDL IDL FFA
Lipoprotein Lipase Deficiency(Type I) • Chylomicrons: • Intestinal lipoprotein, containing mostly triglycerides. • Rapidly degraded by lipoprotein lipase in vasculature • Deficiency produces Type I Hyperlipidemia
Type I Hyperlipoproteinemia(Familial Hyperchylomicronemia) • Autosomal recessive transmission. • Third most frequent cause of pancreatitis • Dietary fats, alcohol, estrogens can cause massive (>100 mmol/L) hypertriglyceridemia • Gene frequency ~1:80 in Lac St-Jean • Heterozygotes present with delayed postprandial triglyceride clearance • Possibly at increased risk of CAD
Lipoprotein Lipase Gene 8q LPL gene 8q22 Asp9Asn Glu188Gly Ans291Ser Ser447Ter
Lipoprotein Lipase Gene and CAD LPL Meta-analysis 29 studies, 20 903 subjects Wittrup HH et al. Circulation 1999;99:2901
Case 2 • Familial Hypercholesterolemia • Heterozygous • Frequency 1:500 (up to 1:80 in Lac St-Jean) • LDL-Receptor gene defect • LDL-C 2x ULN
Familial Hypercholesterolemia • Most frequent genetic disorder associated with premature CAD (3-5%) of patients. • LDL-receptor defects underlie the majority of cases • Defective apolipoprotein B (ligand for the LDL-R) • Third genetic locus identified • CAD develops in men 35-55 years, in women 45-65 years. • Respond to statins (+resins) (+ezetimibe)
Lipoprotein Metabolism LDL-R FFA Liver HL LPL Exogenous Pathway Chylo Remnant Chylomicron Peripheral Cells Free Cholesterol ApoA-I, A-II ApoC-I, C-II, C-III Phospholipids Free cholesterol Intestine X Steroidogenic Cells HL LCAT HDL3 Nascent HDL HDL2 LDL Liver X ApoA-I, A-II ApoC-I, C-II, C-III Phospholipids Free cholesterol CETP PLTP Tg Endogenous Pathway CE 3 Liver HL LPL VLDL IDL FFA
IDL VLDL ApoB ApoE ApoB ApoE Endosome VLDL-R LRP ApoB LDL-R LDL Cholesterol HMG CoA Red ACAT Cholesteryl esters Fatty acids sER Lipoprotein assembly and secretion Bile acids VLDL Hepatic Cell
Lipoprotein Metabolism FH HMZ FFA Liver HL LPL Exogenous Pathway Chylo Remnant Chylomicron Peripheral Cells Free Cholesterol ApoA-I, A-II ApoC-I, C-II, C-III Phospholipids Free cholesterol Intestine X Steroidogenic Cells HL LCAT HDL3 Nascent HDL HDL2 LDL Liver X ApoA-I, A-II ApoC-I, C-II, C-III Phospholipids Free cholesterol CETP PLTP Tg Endogenous Pathway CE 3 Liver HL LPL VLDL IDL FFA
Familial Hypercholesterolemia • LDL-R gene (19p13) (Familial Hypercholesterolemia) • LDL-Receptor Defects • Apo B gene (2q23) (Familial Defective apo B) • Apolipoprotein B Mutations • PCSK9 (proprotein convertase subtilisin/kexin type 9) (1p32) • Autosomal Dominant Hypercholesterolemia • ARH gene (1p35-36.1) (Autosomal Recessive Hypercholesterolemia) • LDL-R internalization defect • LDL Overproduction Defects (1q21)(Familial Combined Hyperlipidemia)
Molecular Causes of Familial Hypercholesterolemia (FH) ApoB: Familial defective Apo B LDL-R: Primary familial hypercholesterolemia ARH: Autosomal recessive familial Hypercholesterolemia PCSK9: Proprotein convertase subtilisin/kexin type 9
HPS Heart Protection Study SIMVASTATIN: MAJOR VASCULAR EVENTS Vascular event Statin (n=10,269) Placebo (n=10,267) Risk ratio and 95% CI Total CHD 914 1,234 Total stroke 456 613 Revascularisation 926 1,185 ANY OF ABOVE 2,042 2,606 24%SE 2.6 reduction (2P<0.00001) (19.9%) (25.4%) 0.4 0.6 0.8 1.0 1.2 1.4 Statin better Statin worse
Cholesterol treatment Trialists(Lancet 2005;366:1267) Proportional reduction in event rate Reduction in LDL-C (mmol/L)
LDL Apheresis 500 Apheresis 400 300 Mean LDL-C (mmol/L) Mean LDL-C (mg/dL) 200 + Atorvastatin 100 1999 1992 1993 1994 1995 1996 1997 1998 Time (years) Genest J. NEJM 1999;341:490
Case 3 Type III HLP(dysbetalipoproteinemia) • Type III HLP • Rare • Tuberous xanthomas and palmar xanthomas • Diagnosis is made on clinical grounds, • Lipoprotein ultra-centrifugation • Apo E phenotype or genotype
Type III Hyperlipoproteinemia • Type III HLP • Dysbetalipoproteinemia, Remnant disease • Apo E2/2 genotype + one other “hit” (unknown for the most part) • Responsive to diet and drug therapy • Accumulation of remnant lipoproteins because of abnormal uptake by the liver • Apo E4/4 associated with Alzheimer’s disease age of onset
Lipoprotein Metabolism Type III FFA Liver HL LPL Exogenous Pathway X Chylo Remnant Chylomicron Apo E2/2 Peripheral Cells Free Cholesterol ApoA-I, A-II ApoC-I, C-II, C-III Phospholipids Free cholesterol Intestine Steroidogenic Cells HL LCAT HDL3 Nascent HDL HDL2 LDL Liver ApoA-I, A-II ApoC-I, C-II, C-III Phospholipids Free cholesterol CETP PLTP Tg Endogenous Pathway CE 3 Liver HL LPL VLDL X IDL Apo E2/2 FFA