ACUTE MESENTERIC ISCHAEMIA
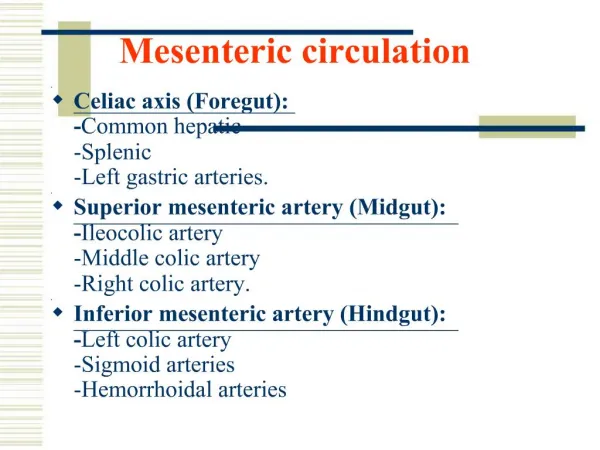
DR. N. WHEELER. ACUTE MESENTERIC ISCHAEMIA. BASIC ANATOMY. Celiac artery, SMA, and IMA supply foregut, midgut, and hindgut, respectively Celiac artery: Supplies lower esophagus, stomach, duodenum, liver, pancreas, and spleen SMA:

ACUTE MESENTERIC ISCHAEMIA
E N D
Presentation Transcript
DR. N. WHEELER ACUTE MESENTERIC ISCHAEMIA
BASIC ANATOMY • Celiac artery, SMA, and IMA supply foregut, midgut, and hindgut, respectively • Celiac artery: • Supplies lower esophagus, stomach, duodenum, liver, pancreas, and spleen • SMA: • Communication between superior and inferior pancreaticoduodenal arteries is an important anastomosis that helps to maintain bowel perfusion in atherosclerotic disease of the mesenteric vessels • Supplies the ileum, cecum, ascending colon, the transverse colon and communicates with the IMA. • Right and middle colic arteries are an important supply of blood to the marginal artery of Drummond
BASIC ANATOMY... • IMA: • Smallest mesenteric vessel • Supplies distal transverse, descending, sigmoid colon, rectum • Rectal branches offer anastomosis between visceral blood supply and the common supply • SMV drains the small intestine, cecum, ascending colon, transverse colon, stomach, pancreas and duodenum • IMV drains descending colon, sigmoid colon, rectum • IMV joins the splenic vein, which then joins the SMV to form the portal vein. The portal vein enters the liver
PATHOPHYSIOLOGY • Insufficient blood perfusion of small bowel or colon may result from: • Embolic (50%) or Thrombotic arterial (25%) occlusion • Thrombotic venous occlusion (10%) • Non-occlusive processes (20%) • Injury severity is inversely proportional to mesenteric blood flow (number of vessels involved, systemic mean blood pressure, duration of ischemia, and collateral circulation) • SM vessels are more frequently involved than the IM vessels (larger diameter and better collaterals with inferior vessels) • Damage may range from reversible ischemia to transmural infarction with necrosis and perforation • Injury complicated by reactive vasospasm in SMA after initial occlusion and Arterial insufficiency causes tissue hypoxia, leading to bowel wall spasm initially(vomiting or diarrhea) • Mucosal sloughing may cause bleeding into the GIT
PATHOPHYSIOLOGY • Minimal abdominal tenderness is present at this stage despite symptoms of intense visceral pain • If ischemia persists disruption of mucosal barrier occurs and bacteria, toxins, and vasoactive substances are released into the systemic circulation • This can cause septic shock, cardiac failure, or multi-organ failure before bowel necrosis actually occurs • With worsening hypoxic damage the bowel wall becomes edematous and cyanotic • Bowel necrosis occurs in 8-12 hours from onset of symptoms • Transmural necrosis leads to peritonism and indicates bad prognosis
ACUTE MESENTERIC ARTERIAL EMBOLISM • Caused by embolism • Typical causes: • Mural thrombi - MI • Atrial thrombi - mitral stenosis and AF, vegetative endocarditis • Aortic thrombi - mycotic aneurysm, thrombi at sites of atheromatous plaques, sites of vascular aortic prosthetic grafts interposed between heart and SMA • Occlusion is sudden and no time to develop compensatory increase in collateral flow • Ischemia is more severe • SMA is most susceptible to emboli due to small angle and greater diameter, with IMA less commonly affected • CDC) Injury Center: special form of AMI due to systemic air embolism in high-energy blast injuries secondary to severe primary blast injury to the lung
ACUTE MESENTERIC ARTERIAL THROMBOSIS • Late complication of preexisting visceral atherosclerosis • Symptoms do not develop until 2 of 3 arteries are stenosed or completely blocked • Slow process of atherosclerotic stenosis before acute occlusion allows time for development of collateral circulation • Thrombus formation results in acute cessation of blood flow to GIT resulting initially in mucosal ischaemia and necrosis causing bloody stools • Bowel wall also becomes necrotic leading to bacterial overgrowth and bowel perforation, sepsis and death • Patients usually have history of atherosclerotis at other sites (eg, CAD, strokes, PVD) or other vascular disease (Aortic Aneurysms, dissections, trauma) • Drops in cardiac output after MI, CCF may cause AMI in pre-existing visceral atherosclerosis • Patients frequently present with history of chronic mesenteric ischemia and symptoms of intestinal angina before acute event
NONOCCLUSIVE MESENTERIC ISCHEMIA • Precipitated by severe reduction in mesenteric perfusion secondary to arterial spasm or decreased cardiac output • Causes: • Cardiac failure • Shock • Use of potent vasopressors in critically ill patients • Bowel perfusion, like cerebral perfusion, is preserved in hypotension therefore NOMI represents a failure of autoregulation • Vasoactive drugs (eg, digitalis, cocaine, diuretics, and vasopressin) may also cause regional vasoconstriction • Gross pathologic arterial or venous occlusions are not observed
MESENTERIC VENOUS THROMBOSIS • Secondary MVT -!>80% result of processes that predispose patients to form clot in mesenteric circulation • Primary MVT occurs in the absence of any identifiable predisposing factor • Causes: • Malignancy • Blood disorders - Sickle cell disease, Protein C & S deficiency • Post surgery - after ligation of the splenic vein, portal vein or SMV • Mechanism for ischemia is a massive influx of fluid into the bowel wall and lumen, resulting in systemic hypovolemia and haemoconcentration • Subsequent bowel edema and decreased venous outflow impedes inflow of arterial blood and leads to bowel ischemia • Much younger population
MESENTERIC VENOUS THROMBOSIS • Symptoms may be present longer • Infarction rarely observed with isolated SMV thrombosis, unless collateral flow in peripheral arcades or vasa recta is also affected • Fluid sequestration and bowel wall edema are more pronounced than in arterial occlusion • Colon rarely involved due to good callateral supply • Abu-Daff et al - 30-day mortality in these patients was strongly linked to colonic involvement in ischemia and to short-bowel syndrome.[26] Lack of anticoagulation also may have been a factor. The 5-year mortality, according to the investigators, was primarily related to short-bowel syndrome.
PROGNOSIS • All-cause mortality 71% (59-93%) • Once bowel wall infarction has occurred the mortality is as high as 90% • Survivors have a high risk of rethrombosis and poor QOL due to short-gut syndrome • Predictors of mortality: older age, hepatic and renal impairment, metabolic acidosis, hypoxia, intramural pneumatosis, and sepsis • Mortality is highest for thrombotic AMI followed by NOMI, embolic AMI and venous thrombotic AMI • Early and aggressive diagnosis and treatment shown to reduce mortality if diagnosis made before onset of peritonitisis • Madrid study - described 21 patients with SMA embolus • Intestinal viability achieved in 100% of patients if symptoms <12 hours, 56% if <12-24 hours, and 18% if > 24 hour
http://www.cdemcurriculum.org/ssm/gi/mesenteric_ischemia/mesenteric_ischemia.php
http://drkeyurbhatt.blogspot.com/2012/12/case-acute-mesenteric-ischemia-due-to.html http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1130-01082010000500007
REFERENCES • Medscape