Download
1 / 35
350 likes | 391 Views
Unusual anterior Uveitis in a Child. Ocular History. 10 year old boy 1/2001: OD>OS red eyes iris thickening , endothelial precipitates , hyphema topical corticosteroids IOP: OD: 40mmHg YAG-iridotomy: unsuccessfull. First Diagnosis. Anterior uveitis of unknown origin. Treatment.

E N D
OcularHistory • 10 yearoldboy • 1/2001: OD>OS • redeyes • iristhickening, • endothelialprecipitates, hyphema • topicalcorticosteroids • IOP: OD: 40mmHg • YAG-iridotomy: unsuccessfull
First Diagnosis • Anterioruveitisofunknownorigin
Treatment • topicalcorticosteroidseveryhour
OcularHistory at Presentation • 6 weeks after firstsymptoms • VA OD 8/20; OS 12/20 • IOP: 18/16mmHg • slitlamp OD: • iristhickening, • endothelialprecipitates, hyphema • Fundus: unremarkable
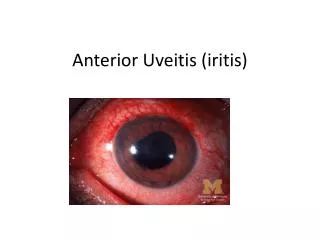
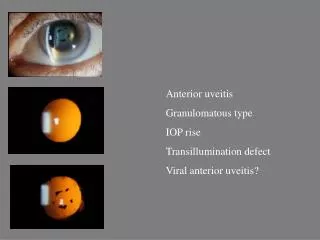
First Presentation - OD • massive granulomatousprecipitates
OcularHistory at Presentation • slitlamp OS • irisprominence at 11 o´clock • mild anteriorchambercells 1+ • fundus: unremarkable
General History • unclassifiedmalformationsyndrome with anal atresia, insufficiencyofthepituitarygland • hearttransplantation at theageof 3 due todilativecardiomyopathy with endocardialfibrosis • several transplant rejections (2000) • Immunosuppression at themoment • Cyclosporin A, Azathioprin
Second Diagnosis • CMV induceduveitis • based on: • CMV mismatch at transplantation • leadingto high IgG- andIgM- antibodytitersagainst CMV
Change of Treatment • systemicganciclovir in addition • repeated negative PCR and PP-65 ruled out active CMV, leadingto • stopofganciclovir • clinicallyandserologicallynoevidencefor sarcoidosis, toxoplasmosis, toxocaraor HIV-infection
Follow up – After 3 Months • angle closure - peripheral iridectomy • severe hyphema • systemiccorticosteroids
HistologyofIrisbiopsy • firstview • lymphocytes • nolymphoma • severeinflammation • secondview: • veryfewmitoticcells • probablylowmalignant non Hodgkin-lymphoma
Irisbiopsy – HE-Staining • polymorphiclymphocyticinfiltration (brown) • Rohrbach et al. Graefe´sArchClinExp Ophthalmol 2004
ImmunohistologyofIrisbiopsy • CD 20 +/ CD3 - lymphocytes
Irisbiopsy- Immunostainig Rohrbach et al. Graefe´sArchClinExp Ophthalmol 2004
Irisbiopsy - EBV • irisbiopsy: positive PCR for EBNA-1 • EBV-load: 5,6 x 10-3 (20 x elevated) • monoclonalrearrangement in the CD2 regionofIg heavy chaingene in cellsofthetumour (IgH-gene)
Gel-Electrophoresis • PCR with primersfortheIg heavy chaingene, hypervariable region • A,B: tumour • L: lengthmarker • P: pos. control • lane 5, 6: neg. control Rohrbach et al. Graefe´sArchClinExp Ophthalmol 2004
Diagnosis • Posttransplantation-Lymphoproliferative Disease (PTLD) • localized NH-lymphoma in children after severeimmunosuppression • nearlyexclusively associated to EBV • interpretationofhistologyknowntobedifficult
Follow up – After 5 Months • low dose CsA, azathioprinestopped • ganciclovirorally • OS: iristumorregressedslightly • OD: iristumorprogressed • high EBV-replication rate in mononuclearbloodcells
Follow up - After 6 Months • radiation (5 x 2.0 Gy/week) • welltolerated • at the end oftheradiation • mild conjunctivitis • partial remissionofthetumor
Follow up - After 8-12 Months • completeremissionoftheoculartumor • hypotonicsituation • cataract with convergentsquint • still very high EBV titers
Follow Up – After 13 Months • viral load half ofthebeginning • still consistant with persistantactive EBV-infection • foscarnetstarted • after a fewweeks: • viral loadevenhigherthanbeforebeginofthefoscarnettherapy • probably high riskformorelymphoma
Follow Up – After 17 Months • collectionof EBV-infected B-cellsfromthepatient • generationofpatientsownspecificcytotoxic anti-EBV T-cells • Center for Gene and Cell Therapy Houston TX, USA
Follow Up – After 22 Months • anti-EBV Treatment • reinfusionofthe T-cells in 3 portions • reductionofthe EBV load • freeofcells in theanteriorchamber
Last Control – After 32 Months • VA: OD: handmovements, OS: 16/20 • OU: • clearcornea, no AC cells • noiristumors • IOP 5 and 10 mmHg • OD: densecataract, surgeryplanned • then lost for follow-up
Posttransplantation Lymphoproliferative Disorder • all agegroups • after transplantationofkidney, liver, heart, lungorbonemarrow • incidence ca. 2-3 % • latencyfewweeksto 3 years • highestincidenceprobably in thefirstyear after transplantation
Posttransplantation Lymphoproliferative Disorder • specialentity, no simple lymphoma • 3 variants • circumscribedlesion, typicallylaterthan 1 year after tranplantation, oftenlocalized in the CNS, gastrointestinal tractorsalivaryglands • benign, selflimitingdiseaseresemblingmononucleosis • malignantwidespreadlymphoproliferation with high mortality
Ocular PTLD • Brodsky et al 1991 • untilnow 14 cases (50% with syst. disease) • 7 with irisnodules • 2 with irisnodulesand subretinal mass • 1 with widespreaddisease (uvea, retina, opticnerve,orbit) • 1 vitritis,1chorioretinitis,1 anterioruveitis • 1 orbital mass
HistologyofOcular PTLD • proliferationof B-cellsand/orplasmacells • proliferationof T-cells in 10% • polyclonalormonoclonal
Roleof EBV • most PTLD causedby a chronic EBV-infection • EBV negativ recipientsare at higherriskthan positive • detectable in thetumorandbloodmonocytes • anti-T-cell treatmentespeciallydangerous • CMV-infectionelevatesriskfor PTLD • therapy: reductionof IS, increaseantivirals
Conclusion • PTLD incidence ca. 2-3% • diagnosis: historyof solid organtransplantation • canaffecttheeye • irisnodules • uveitis • therapy: • reductionofimmunosuppresion • virustatics • generationofown anti-EBV cytotoxic T-cells