Download
1 / 37
460 likes | 1.38k Views
Immunology of Uveitis (Autoimmune Uveitis). Dr S.H. Zarkesh Department Of Immunology, Medical School, Isfahan University Of Medical Sciences, Isfahan, I.R.IRAN. email: s.h.zarkesh@sheffield.ac.uk Website: www.shef.ac.uk/hamid. Autoimmune Disease Definition.

E N D
Dr S.H. ZarkeshDepartment Of Immunology, Medical School, Isfahan University Of Medical Sciences, Isfahan,I.R.IRAN email: s.h.zarkesh@sheffield.ac.uk Website: www.shef.ac.uk/hamid
Autoimmune DiseaseDefinition • Ehrlich referred to this phenomenon as horror autotoxicus • Specific adaptive immune response directed against self antigen(s) with loss of tolerance, usually peripheral, not central • Trigger(s) is usually unknown. • Immune response involves both environmental and genetic factors • female predominance
Autoimmune DiseaseCharacteristics • remissions and exacerbations • organ specific or organ non-specific • persistence of antigen due to lack of clearance • tissue damage is produced by: • antigen specific cytotoxic T cells (CD8+) • antigen-non-specific NK cells and macrophages • immune complexes • autoantibodies , and/or • granulocytes
Possible Pathogenic Defects Human Autoimmunity • Multiple genes are involved in human autoimmune disease e.g. IDDM (type I), especially involving the MHC • Defects in several of these genes may: • disrupt multiple tolerance pathways and • contribute in an additive or synergistic way to these polygenic diseases • Important individual roles for: • Fas-FasL • IL-2/IL-2R (AICD) • B7-CTLA-4 interaction This suggests that each role may be involved in different pathways of tolerance, perhaps for distinct types of self antigens
Human Autoimmune Diseases • Organ Non-Specific Diseases • SLE (systemic lupus erythematosus) • RA (rheumatoid arthritis)
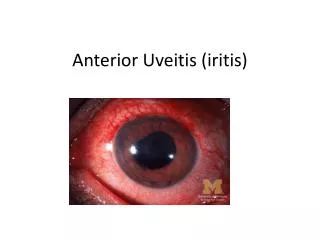
Autoimmune uveitis • can be • part of a systemic autoimmune syndrome involving multiple tissues, such as Behc¸et’s disease, systemic sarcoidosis. • In other diseases the eye may be the only target, such as in idiopathic uveitis, birdshot retinochoroidopathy, and sympathetic ophthalmia
Uveitic diseases are believed to have an • autoimmune component supported by: • 1) lack of a known infectious trigger • 2) and by frequent presence of immunological responses to retinal proteins. • 3) Many uveitic diseases show strong • associations with particular human leukocyte antigen (HLA) haplotypes.
The model of experimental autoimmune uveitis/uveoretinitis • (EAU) • In rodents is used as an animal model for • human uveitis. • The classical model of EAU is induced by • active immunization with a retinal antigen (Ag) emulsified in • complete Freund’s adjuvant (CFA), a mineral oil supplemented • with heat-killed mycobacteria. • In all but the most • susceptible mouse and rat strains, an injection of pertussis • toxin must be given as an additional inflammatory stimulus
uveitogenic stimulus that is thought to trigger uveitis in • humans, which is believed to involve • 1) an exposure to a retinal or cross reactive Ag, combined with an infectious event that • provides innate inflammatory danger signals. • 2) Uveitogenic retinal proteins include • retinal arrestin (soluble Ag), • interphotoreceptor • retinoid-binding protein (IRBP), • rhodopsin, • recoverin, • phosducin, • and retinal pigment epitheliumderived RPE-65.
Of the available models, • the mouse model of EAU induced with retinoid-binding protein (IRBP) is the best characterized and the most widely used. • The typical histological appearance of EAU resembles that of human uveitis, with inflammatory infiltrates in the vitreous, retina, • and choroid and damage to the photoreceptor cell layer. You can see the details of this phenomenon in next slide.
Adaptive/effector T cells from EAU-induced animals can pass the disease to naı¨ve, genetically compatible recipient • animals by adoptive transfer. • The donor T cells are activated with the immunizing Ag in vitro and are infused into recipient animals. • The recipients develop a destructive disease • rapidly, usually within a week.
Recently, an alternative model to IRBP/CFA-induced uveitis have been developed . • Dendritic cells (DC) are professional • Ag-presenting cells capable of stimulating naı¨ve T • cells, and are likely to be the main Ag-presenting cells in the early stages of EAU induction. • A model of EAU was developed • by injection of matured splenic DC loaded with the • major uveitogenic peptide of IRBP into naı¨vewild-type mice.
Compared with the classical EAU model induced by active immunization with IRBP or its peptide in CFA, • 1) duration of the disease is shorter, the pathology • appears to be less severe, • 2) and the inflammatory infiltrate has a predominantly granulocytic rather than mononuclear cell composition. Importantly, • 3) EAU elicited with Ag-pulsed DC is not only clinically distinct from CFA induced EAU, but also is driven by unique effector mechanisms • . This model may offer new insights into the heterogenous nature of human uveitis.
Cytokines play an important role in maintaining lymphocyte • homeostasis under conditions of health and disease. • Intraocular expression of cytokines has been studied in patients • with uveitis, with reports of increased levels of inflammatory • cytokines and decreased levels of regulatory • Cytokines. • The roles of various cytokines and how they affect the • critical checkpoints of uveitis, as studied in animal models • and to a lesser extent in patients, are shown in Table 1 and • discussed in the following slides.
Th1 Cells and Cytokines in Uveitis(IFN-gamma and IL-12) • IL-12, composed of 2 heterodimeric subunits, p35 and p40 • is produced by DC and macrophages, is a key Th1-inducing • cytokine. • The roles of IL-12 and of IFN-g, the main signature • cytokine of the Th1 lineage, have been intensively studied in • EAU models in the 1990s. • At that time, the Th17 subset • (discussed ahead) had not yet been described, and the Th1 • subset was thought to be the major pathogenic effector T cell • subset in uveitis. • An IRBP-specific uveitogenic T cell line • polarized to the Th1 phenotype in the presence of IL-12 and • producing massive amounts of IFN-g was highly uveitogenic • in naı¨ve recipient animals.
Emerging Treatments of Clinical UveitisTargeting Cytokines and Their Receptors • Established therapies for uveitis are based largely on • nonspecific immunosuppression (corticosteroids, antimetabolites,andalkylating agents). • However, because of the severe side effects of these treatments, it is important to develop new approaches based on increased understanding • of basic disease mechanisms, so as to intervene more specifically in the pathogenic processes
Although involvement of many cytokines has been demonstrated in experimental Uveitis as shown in the next slide.
One of the hazards involves the pleiotropic • nature of some cytokines and the possibility to elicit • unexpected reactions. As an example, a clinical trial to treat • multiple sclerosis that was undertaken on the basis of early • data in mice showing that IFN-g can have protective effects • in EAE (similarly to EAU) resulted in exacerbation of the • disease and had to be stopped
CsA was first shown to have a therapeutic effect in the rat EAU model before going to clinical trials. The macrolides FK-506 (tacrolimus) and rapamycin (sirolimus) also target the IL-2 signaling pathway and are effective for some types of uveitis
More recent studies have examined IL-2 receptor-directed therapy with monoclonal antibodies (daclizumab) as an approach to target activated T cells. This therapy has shown efficacy in advanced clinical trials.
Interestingly,the possibility that such treatment might actually aggravate T cell-mediated autoimmunity because IL-2 is necessary for the maintenance and activity of Treg cells (at least in mice) was not fulfilled.
The mechanism behind the therapeutic effects of daclizumab is complex and incompletely understood, but includes an enhancement in CD56-bright NK cells with inhibitory function
Since the eye is a small and relatively closed organ, local therapies in the eye are an attractive approach that can obviate systemic side effects. • Intravitreal injections or implants are already in use for such local therapies, and biological • products can also be delivered into the eye. • Locally produced IL-10 has been shown to be beneficial in animal models
This • opens the possibility for intraocular injection of other antiinflammatory • molecules, such as IL-27 and IL-35, or even • in vitro generated Treg cells. For this purpose, it will be important • to develop minimally invasive and highly efficient • local drug delivery approaches
Anterior Uveitis Topical: Steroid drops Cycloplegics Systemic: Corticosteroids Steroid sparing agents Posterior Uveitis Local: Periocular steroid injections Systemic: Corticosteroids Steroid sparing agents Approach to Treatment