Download

1 / 37
370 likes | 510 Views
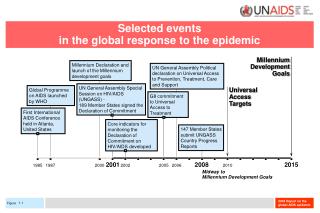
Erfolge und Stolpersteine auf dem Weg zu Universal Access. MDG 6 to Road 2015. Achieve, by 2010, universal access to treatment for HIV/AIDS for all those who need it. MDG 6. Combat HIV/AIDS, Malaria and Other Diseases. Target 6.A:

E N D
Erfolge und Stolpersteine auf dem Weg zu Universal Access MDG 6 to Road 2015 Achieve, by 2010, universal access to treatment for HIV/AIDS for all those who need it
MDG 6 Combat HIV/AIDS, Malaria and Other Diseases Target 6.A: Have halted by 2015 and begun to reverse the spread of HIV/AIDS 6.1 HIV prevalence among population aged 15-24 years 6.2 Condom use at last high-risk sex6.3 Proportion of population aged 15-24 years with comprehensive correct knowledge of HIV/AIDS6.4 Ratio of school attendance of orphans to school attendance of non-orphans aged 10-14 years Target 6.B: Achieve, by 2010, universal access to treatment for HIV/AIDS for all those who need it 6.5 Proportion of population with advanced HIV infection with access to antiretroviral drugs Target 6.C: Have halted by 2015 and begun to reverse the incidence of malaria and other major diseases
Es gibt Erfolge.. UNAIDS Report 2010
Prävention der sexuellen Übertragung Signifikante Reduktion~ 25% der Prävalenz im Alter von 15-24 in 10 Hochprävalenz Ländern Reduktion verknüpft mit Verhaltensänderung Späteres sexuelles Debut Weniger gleichzeitige sexuelle Partner Höhere Rate an Kondom Nutzung The International Group on Analysis of Trends in HIV Prevalence and Behaviours in Young People in countries most affected by HIV, IAC July 2010 Trends in HIV prevalence and sexual behaviour among young people aged 15-24 years
Kennen Sie das 2:5 Problem ?
Vorsicht, Stolperstein: Auf 2 HIV infizierte Menschen, die neu mit der Behandlung beginnen, kommen immer noch 5 (4?) neue Infektionen UNAIDS Report /TUAPR 2010 Neuinfektionen ca 2.6 Mio, (2009) neu unter Behandlung ca 1.2 Mio (2008-2009)
Michel Sidibé: Vorwort zum UNAIDS Report 2010
Treatment 2.0 • Maximisingefficiencyandeffectivenessof HIV treatment • Focus on fivepriorities • Optimisingdrugregimens • Advancingpoint-ofcareandothersimplifiedplatformsfordiagnosisandmonitoring • Reducingcost • Adaptingdeliverysystems • Mobilisingcommunities Hirnschall, Schwartländer , Lancet Feb 2011
Der deutsche Beitrag, die deutsche Perspektive • Politik • Wissenschaft • Persönliches Engagement
Politik • Lobbyarbeit • Aktionsbündnis AIDS, Deutsche Aidsstiftung und andere Partner • Öffentlichkeit herstellen – DAIG UA web site • Brief anteilige Finanzierung des Globalen Fonds
9000 8000 7000 US$ million 6000 5000 4000 PEPFAR 3000 2000 1000 0 Total annual resources available for HIV 1986‒2007 13700 million USD 8297 Signing of Declaration of Commitment on HIV/AIDS, UNGASS World Bank MAP launch UNAIDS Less than US$ 1 million 1623 Global Fund 292 257 212 59 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2007 * Sources: 2007 data: Keiser Family Foundation (2009) 1996-2005 data: Extracted from 2006 Report on the global AIDS epidemic (UNAIDS, 2006) & 1986-1993 data: AIDS in the World II. Edited by Jonathan Mann and Daniel J. M. Tarantola (1996) Courtesy Anna Mia Ekstroem
Early initiation of ART?Umsetzung der neuenLeitlinie der WHO am Beispiel Malawi 25 % Unterfinanzierung des gegenwärtigenProgramms Ca 45% mehrPatienten “in need” HöhererPersonalbedarf HöhereBehandlungskostenfür alternatives Regime: d4T/3TC/NVP- 85 $ (224$) pro Kopf and Jahr AZT/3TC/NVP-151$ (288$) TDF/3TC/EFV-240$ (373$)
Early initiation of ART? Courtesy Sam Phiriand Malawi HIV Program
Projizierte Ergebnisse des Globalen Fonds in Abhängigkeit vom Finanzvolumen 2011-2013 in Klammer : geschätzter Anteil des abgedeckten Bedarfs Quelle: www.theglobalfund.org/documents/replenishment/2010/Resource_Scenarios_en.pdf
Wissenschaft /Forschung • Public Health Forschung • Gesundheitssystem Fragen wie Finanzierung • Humane Ressourcen (Fachkräftemangel) • Nachhaltige Strukturen für qualitative gesicherte Versorgung • Klinische , epidemiologische Forschung • Optimierung der Medikamente/ Resistenzentwicklung • Prävention der Mutter Kind Übertragung • Therapie bei Ko-Infektionen/ Begleiterkrankungen • Umsetzung von Studienergebnissen z.B. diskordante Paare
Probleme der Gesundheitsdienste • Personal • Management • Arzneimittel-versorgung • Finanzen
Management z.B. Dokumentation Real time touch Screen Eingabe Gut geordnetes Akten basiertes System bei einer NGO bzw. in einem Missionskrankenhaus
Dokumentation Multiple Anforderungen von Geber Organisationen Mehrfache Einträge erforderlich Mangelhafte Ordnung Staatliche Gesundheitseinrichtung
Management: Retention in Care Fox , Rosen, TropMedand International HealthVol 15 Suppl 1-pp 1-15, June 2010 Based on 33 sourcesdescribing 39 cohortsand 226 307 patients
Mchukwi Mission Hospital • Electronic data entry (Plus 1 staff responsible!) allows analysis: • “Currently on ART” over “ever started” in Mchukwi 566 /866 (65%) • Of the 300 no longer on ART • 67 confirmed deaths (7,7%) • 108 lost to follow up (12,4%) • 62 reason unknown (7,2%) • 16 stopped (1,8 %) • 47 transfer out (5,4%) • Growth of ART program factor 1,6 • Stock out of ART compensated by program partner * average since previous assessment **average over the past quarter
Wer kann und soll HIV behandeln? Nurse versus doctormanagementof HIV infectedpatientsreceiving antiretroviral therapy (CIPRA-SA): a randomised non-inferioritytrial Lancet 2010, 376:33-40
Wie Arzneimittelversorgung sicherstellen? • Verbessertes Supplychainmanagement • Bezahlbare Preise – patent pool? Innovative Finanzierungsmechanismen • Ausschöpfung politischer Rahmenvorgaben TRIPS • Qualitätssicherung - prequalification
Fluctation in patientrecruitmentto ART associatedwithirregulardrugsupply
Stigma und Diskriminierung • Reduziert durch Zugang zur Behandlung „Normalisierung“ • Fortbestehend besonders in Bezug auf bestimmte vulnerable Gruppen • Führen zu verspäteten Zugang zur und Unterbrechung der Behandlung
Organisation dieses Workshops • Geplante Datenbank zu HIV Aktivitäten in Hochprävalenzländern • Deutsche Kliniken und Institute in ESTHER Partnerschaften • Kooperation mit AIDS-Stiftung • Mitarbeit beim Aktionsbündnis gegen AIDS
Bilanz Erfolge Stolpersteine Schwache Gesundheitssysteme Austrocknung der Finanzen, „Donorfatigue“ Mangel an Fachkräften und etablierten alternativen Versorgungsmodellen Versorgungslücken „Stock outs“ , Gefahr der Resistenzbildung Teure Second line Medikamente Fortbestehen von Ausgrenzung insbesondere bei Gruppen wie MSM, Drogennutzern „Präventionslücke“ (2:5) • Erhebliche Steigerung des Zugangs zu Prävention, Behandlung und Versorgung seit 2002 • Global Fund, PEPFAR, Zivilgesellschaftliches Engagement u.a. • Bis dato ungekannte Steigerung der Mittel für Gesundheit in armen Ländern • Behandlungserfolge in RLS vergleichbar mit „westlicher“ Erfahrung • Rückgang von Diskriminierung • Fortschritte bei der Prävention
Die Zielvorgabe zu erreichen, heisst • Gesundheitssysteme stärken • Lösungen für den Personalmangel • Bezahlbare Medikamente und Diagnostika • Finanzierung sicherstellen lokal und international • Vorurteile, Stigma und Diskriminierung abbauen • Weltweite Lobbyarbeit, auch als Individuum • Angemessenen deutschen-österreichischen Beitrag leisten
Es gibt noch viel zu tun auch von deutsch-österreichischer Seite!Danke für die Aufmerksamkeit Dr. Florian Neuhann , Universitätsklinikum Heidelberg, Institut für Public Health Sprecher der Sektion