Download
1 / 47
510 likes | 874 Views
Lipids and Lipoproteins. Roger L. Bertholf, Ph.D. Associate Professor of Pathology Director of Clinical Chemistry & Toxicology. Classification of lipids. Fatty acids (palmitic, linoleic, etc.) Glycerol esters (triglycerides) Sterols (cholesterol, hormones, vitamin D)

E N D
Lipids and Lipoproteins Roger L. Bertholf, Ph.D. Associate Professor of Pathology Director of Clinical Chemistry & Toxicology
Classification of lipids • Fatty acids (palmitic, linoleic, etc.) • Glycerol esters (triglycerides) • Sterols (cholesterol, hormones, vitamin D) • Terpenes (vitamins A, E, K) • Sphingosine derivatives (sphingomyelin)
Fatty acids • Even-numbered fatty acids predominate • The most common saturated fatty acids are palmitic (16:0) and stearic (18:0), but unsaturated fatty acids are more common in nature Lauric acid (C12, 12:0, n-dodecanoic acid)
Unsaturated fatty acids • Double bonds in fatty acids are nearly always cis Palmitoleic acid (16:19, 9-hexadecanoic acid)
Essential fatty acids • Mammals can synthesize saturated and mono-unsaturated fatty acids. • Linoleic (18:2) and linolenic (18:3) fatty acids cannot be synthesized, and therefore must be obtained from the diet (plants). • Both are required for the biosynthesis of prostaglandins
Clinical importance of fatty acids • Fecal fatty acids are sometimes measured to detect malabsorptive and pancreatic disorders—the test is mostly considered obsolete • Serum free fatty acids help distinguish between hyperinsulinemic hypoglycemia (FFA normal) and disorders of fatty acid oxidation (FFA elevated and negative ketones)
Glycerol esters (acylglycerols) • Triglycerides are the most abundant family of lipids in plant and animal cells, and are major components of the the human diet Glycerol Triglyceride
Measuring triglycerides (reference method) • Triglycerides are extracted into chloroform prior to analysis Triglycerides fatty acids + glycerol KOH formic acid + formaldehyde Periodate chromogen =570 nm chromotropic acid
Lipase Glycerokinase ATP Glycerol + FFAs Glycerophosphate + ADP Measuring triglycerides (enzymatic method) Triglycerides Glycerophasphate oxidase Dihydroxyacetone + H2O2 Quinoneimine dye max 500 nm Peroxidase
Sterols (cholesterol) • Sterols are steroid backbones that have a hydroxyl group at position 3 and a branched aliphatic chain of 8 or more carbons at position 17
Cholesterol biosynthesis • About 2% (approximately 1 g) of total body cholesterol is replenished each day • Dietary sources account for less than half • Cholesterol is synthesized from Acetyl CoA • 90% of in vivo synthesis occurs in the intestine and liver (although all cells have the capability) • Absorption of dietary cholesterol appears to have a maximum of approximately 1 g/day
“Statin” drugs inhibit this enzyme Cholesterol biosynthesis Acetyl-CoA 3-Hydroxy-3-methylglutaryl-CoA HMG-CoA reductase Squalene Mevalonate Cholesterol + Lecithin Cholesterol ester LCAT
Measuring cholesterol by L-B • The Liebermann-Burchard method is used by the CDC to establish reference materials • Cholesterol esters are hydrolyzed and extracted into hexane prior to the L-B reaction
Cholesteryl ester hydroxylase Cholesterol Cholesterol oxidase Choles-4-en-3-one + H2O2 Phenol 4-aminoantipyrine Peroxidase Quinoneimine dye (max500 nm) Enzymatic cholesterol methods Cholesterol esters • Enzymatic methods are most commonly adapted to automated chemistry analyzers • The reaction is not entirely specific for cholesterol, but interferences in serum are minimal
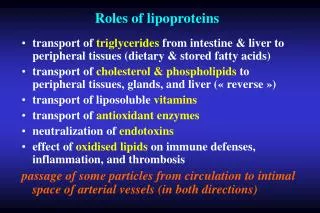
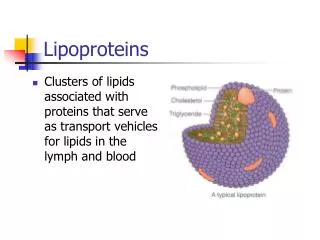
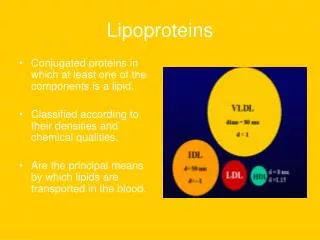
Lipoproteins • In order to be transported in blood, lipids must combine with water-soluble compounds, such as phospholipids and proteins.
Appearance of hyperlipidemia • Standing Plasma Test for chylomicrons • Plasma is placed in refrigerator (4°C) overnight • Chylomicrons accumulate as floating “cream” layer • Chylomicrons in fasting plasma are abnormal
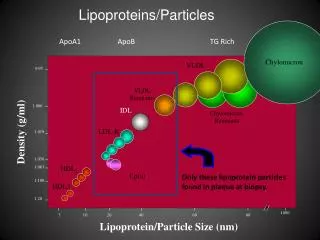
Pre- - + Lipoprotein electrophoresis • LEP is no longer a common laboratory test • Standing plasma test for chylomicrons • Total cholesterol, TG, HDL, and LDL can be measured directly Migration Chylomicrons LDL IDL VLDL Lp(a) HDL
Dextran sulfate HDL, IDL, LDL, VLDL HDL + (IDL, LDL, VLDL) Mg++ Measuring HDL cholesterol • Ultracentrifugation is the most accurate method • HDL has density 1.063 – 1.21 g/mL • Routine methods precipitate apolipoprotein B with a polyanion/divalent cation • Includes VLDL, IDL, Lp(a), LDL, and chylomicrons • Newer automated methods use a modified form of cholesterol esterase, which selectively reacts with HDL cholesterol
Indirect LDL cholesterol • Friedewald formula assumes that all cholesterol is VLDL, LDL, and HDL lipoproteins • Chylomicrons are usually low in normal, fasting subjects, and IDL and Lp(a) are usually insignificant contributors to total cholesterol • Since VLDL is 55% TG and 12% Chol: [LDL Chol] = [Tot Chol] – [HDL Chol] – [TG]/5
Direct LDL cholesterol • Older direct methods for LDL involved precipitation with heparin or polyvinyl sulfate • Newer methods involve precipitation of VLDL, IDL, and HDL with polyvalent antibodies to Apo A and Apo E • LDL is almost exclusively Apo B-100
Direct vs. Indirect LDL • The Friedewald equation assumes that chylomicrons, IDL, and Lp(a) are not significant • Non-fasting specimens can have chylomicrons • TG > 400 mg/dL indicates the presence of chylomicrons (or remnants) • Type III hyperlipidemia is characterized by high -VLDL, which has a 3:1 TG:C ratio
Apolipoproteins • The protein composition differs from one lipoprotein class to another, and the protein constituents are called Apolipoproteins
Functions of apolipoproteins • Activate enzymes involved in lipid metabolism (LCAT, LPL) • Maintain structural integrity of lipid/protein complex • Delivery of lipids to cells via recognition of cell surface receptors
A A C,TG C,TG C E B B Chylomicron C,TG E B Cholesterol metabolism (exogeneous) Dietary cholesterol, triglycerides Apo-C, E from HDL Endothelium LPL Hepatocyte B/E receptors Chylomicron remnant
C,TG E B Cholesterol metabolism (endogeneous) Endothelium C,TG LPL C E B VLDL Hepatocyte B-100 receptors C B LDL IDL
Dyslipoproteinemias • Causes can be primary or secondary • Secondary causes include starvation, liver disease, renal failure, diabetes, hypothyroidism, lipodystrophies, drugs • Primary causes of hyperlipidemia: • Increased production • Defective processing • Defective cellular uptake • Inadequate removal
Dyslipoproteinemias • Hyperchylomicronemia • LPL deficiency • Apo C-II deficiency
A A C,TG C,TG C E B B Chylomicron C,TG E B Hyperchylomicronemia Dietary cholesterol, triglycerides Apo-C, E from HDL Endothelium LPL • Chylomicrons • Triglycerides • HDL • LDL Hepatocyte B/E receptors Chylomicron remnant
Dyslipoproteinemias • Hyperchylomicronemia • LPL deficiency • Apo C-II deficiency • Hyperbetalipoproteinemia • Overproduction of VLDL • Enhanced conversion of VLDL to LDL • LDL enriched with cholesteryl esters • Defective LDL structure • Decreased LDL receptors
C,TG E B Hyperbetalipoproteinemia Endothelium C,TG LPL C E B VLDL Hepatocyte B-100 receptors C • LDL Normal TG B LDL IDL
Dyslipoproteinemias • Combined hyperlipoproteinemia • Normal LDL receptors • Overproduction of VLDL and Apo B-100
C,TG E B Combined hyperlipoproteinemia Endothelium C,TG LPL C E B VLDL Hepatocyte B-100 receptors C • LDL Normal TG B LDL IDL
Dyslipoproteinemias • Combined hyperlipoproteinemia • Normal LDL receptors • Overproduction of VLDL and Apo B-100 • Dysbetalipoproteinemia • Both cholesterol and triglyceride elevated • Mutant form of Apo E
A C,TG B Chylomicron Dysbetalipoproteinemia Dietary cholesterol, triglycerides Apo-C, E from HDL A Endothelium C,TG LPL C E B Cholesterol • TG C,TG E B Hepatocyte B/E receptors Chylomicron remnant
Dyslipoproteinemias • Familial hypercholesterolemia • Defect in LDL receptor • Absent • Defective • Incidence = 1:500
C,TG E B Familial hypercholesterolemia Endothelium C,TG LPL C E B VLDL Hepatocyte B-100 receptors C LDL • or n TG HDL B LDL IDL
Dyslipoproteinemias • Familial hypercholesterolemia • Defect in LDL receptor • Absent • Defective • Incidence = 1:500 • Familial defective Apolipoprotein B-100
Familial hypercholesterolemia Endothelium C,TG LPL C E B VLDL Hepatocyte B-100 receptors C C,TG or n LDL E B B LDL IDL
High cholesterol, high LDL • Diet/Lifestyle • 2° to hypothyroidism or nephrotic syndrome (disruption of Apo-B metabolism) • Polygenic: (means we don’t know) • Familial hypercholesterolemia • Familial defective Apo-B • Rare disorders
High TG, normal cholesterol • Diet/Lifestyle • 2° to diabetes, thiazide diuretics, Cs, beta-blockers, CRF/Nephrotic syndrome • Familial hypertriglyceridemia (etiology unknown) • ApoC-III excess (interferes with LPL) • LPL deficiency • ApoC-II deficiency
High cholesterol, TG • Obesity • 2° to steroids, Cs, hypothyroidism, CRF • Familial combined hyperlipidemia (multifactorial) • Peroxisome proliferator-activator receptor • Dysbetalipoproteinemia (Type III) • Hepatic lipase deficiency (rare)
Low cholesterol, low/normal HDL • Abetalipoproteinemia (ApoB degraded after synthesis causes fat malabsorption) • Hypobetalipoproteinemia (genetically defective ApoB) • Chylomicron retention disease (unknown cause)
Low HDL • Lifestyle • 2° to steroids, beta-blockers, progestogens • Familial hypoalphalipoproteinemia (ApoA-I, C-III, or A-IV defects) • ApoA-I variants • Tangier disease (enhanced HDL degredation) • LCAT deficiency
High HDL • Lifestyle (ethanol) • 2° to phenytoin, phenobarbitol, rifampicin (p-450 inducers) and estrogens • Cholesteryl Ester Transfer Protein defects