Download
1 / 18
200 likes | 330 Views
RESEARCH EVIDENCE ON INDWELLING URETHERAL CATHETER CARE. Francine M Cheater Professor in Public Health Nursing. Urinary Catheters. Indwelling urinary catheters (short or long-term use) Intermittent (self) catheterisation External collecting devices Supra-pubic catheterisation.

E N D
RESEARCH EVIDENCE ON INDWELLING URETHERAL CATHETER CARE Francine M Cheater Professor in Public Health Nursing
Urinary Catheters • Indwelling urinary catheters (short or long-term use) • Intermittent (self) catheterisation • External collecting devices • Supra-pubic catheterisation
Medical Necessity IDC Patient preference
IDC PREVALENCE • Hospital- short term use10-12% • Long term care facilities 16-18% • Home- long term use 4% Acute median 4 days Long termmedian 4 years
RESEARCH • Complications +++ • Specific Procedures ++ • Principles of management in hospital/home ++ • Evaluation of interventions + • Miscellaneous e.g. patient education, economic evaluations
COMPLICATIONS 70-90% patients with LT catheters experience 1 or more recurrent problems-many are secondary to UTI • Urinary tract infection • Pain and discomfort • Leakage of urine • Blockage
UTI • UTI- 105 colony forming units of single species of bacteria/ml urine • In hospital 44% patients with IDC developed bacteriuria within 3 days of catheterisation (UTIs account for 30% of all hospital acquired infections) • Within 2.5 weeks-90% will have bacteriuria (Risks greater for patients with severe underlying illness, catheter induced UTI contributes directly to morbidity and mortality).
UTI • The duration of catheterisation -most important risk factor • Disrupting the closed drainage system (e.g.poor practices when emptying bag/changing bag) presents risk of contamination, cross infection • Use of gloves and/or alcohol rinse and single use of disposable containers to empty bags risk of cross infection. Hand washing alone ineffective. • Optimum time to change bags ?
UTI • Bacteria colonise surface of catheter and drainage bag-produce “biofilm”. Some catheter materials may be less prone to colonisation (e.g. hydrogel coated or silicon Vs. silicon/teflon/latex coated) • Antibiotic therapy for uncomplicated asymptomatic UTI in catheterised patients not effective and could lead to antibiotic resistance • Perineal cleansing vs. usual care
LARGE CATHETERS (Over 16 Ch) -Leakage/bypassing (upto 89% patients with LT catheter) -Trauma - bladder neck -Pain
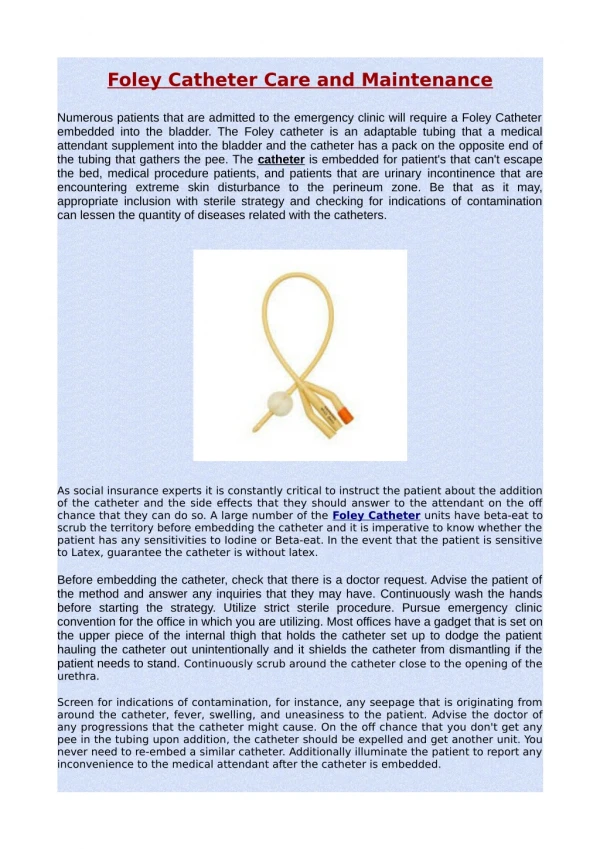
Selection of Catheter • Consensus: optimal size 12-16 males and 12-14 females • Leakage associated with use of balloon size over 10mls • Catheter Material (hydrogel coated and full silicone less likely to encrust) • New materials developed all the time, catheter must fit needs of patient
DRAINAGE BAG/CATHETER VALVES • CATHETER CLAMPING
Blocking • Common (40-87%) with long term catheter use, more common in females, those with poor levels of mobility & high Ph urine values and ammonia concentrates • Caused by: bladder spasm, twisted catheter tube or faecal impaction BUT main reason is encrustation
Blocking • Bladder washouts (dissolve or flush out mineral deposits blocking catheter) • Evidence of effectiveness of using washouts mixed • Weak acidic solution/mandelic acid effective in encrustation in laboratory tests • Saline irrigations not effective • More research needed but bladder washouts may be useful in selected patients • Alternative is to remove catheter and replace
Bladder installations/irrigation • Fluid intake • Antibiotics/antiseptics • Principles of catheter care
Patient perceptions • Patient/carer education
CONCLUSIONS • Considerable research ( controlled trials) to inform practice • Challenge now to implement what we know into practice