Download
1 / 11
160 likes | 541 Views
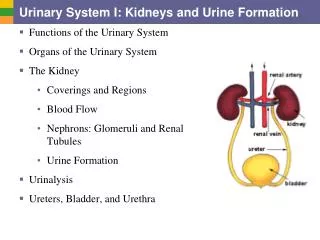
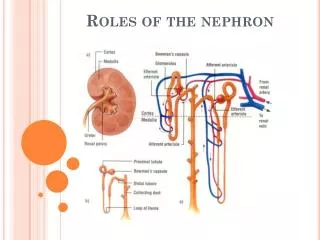
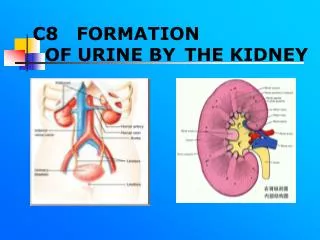
Urine Formation in the Nephron. Urine Formation in the Nephron : four main processes 1. Glomerular filtration renal artery (afferent arteriole) carries blood into the nephron enters the glomerulus , a knot of capillaries inside Bowman’s capsule

E N D
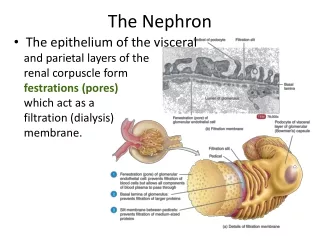
Urine Formation in the Nephron: four main processes 1. Glomerular filtration renalartery (afferent arteriole) carries blood into the nephron enters the glomerulus, a knot of capillaries inside Bowman’scapsule walls of the glomerulus are a filtration device -impermeable to proteins, other large molecules and red blood cells, which remain in the blood -permeable to water, small molecules, ions and urea, which pass through the walls and into Bowman’s capsule; this fluid is called filtrate
blood in the glomerulus is under a great deal of pressure, which provides the force for filtration See Fig. 10.6 pg. 450 glomerular walls are also porous, which allows water and most dissolved substances in the blood plasma, including glucose, amino acids and salts to pass easily through the capillaries and into Bowman’s capsule See Fig. 10.5 pg. 449 essentially the filtrate is identical to blood plasma, minus blood proteins and red blood cells (See Table 10.1 pg. 451), and about 180 L of glomerular filtrate is produced daily
2. Tubular reabsorption filtrate moves into the proximalconvolutedtubule (pct) cells of the pct contain many mitochondria, which provide the ATP needed to pump Na+, K+, glucose, amino acids and other solutes back into the blood negatively charged ions follow along passively, and water moves back into the blood by osmosis, following the concentration gradient created by the pumping of the solutes out of the tubule See Fig. 10.7 pg. 451 substances move back into the bloodstream for reuse in the body
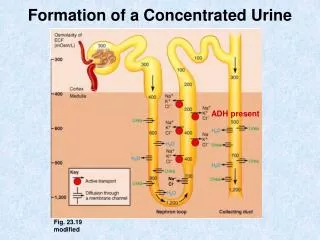
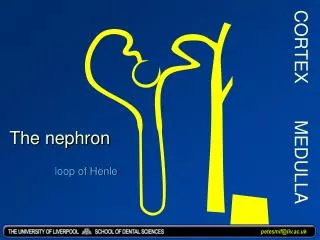
filtrate now moves into the loopofHenle, which is in the medulla cells of the descending loop of Henle are permeable to water and only slightly permeable to ions salty environment of the medulla means water can move out of the tubule and into the capillaries by osmosis See Fig. 10A pg. 452 as water moves to the base of the loop of Henle, Na+ becomes more concentrated due to the loss of water; most concentrated at the base cells of the ascending loop are now impermeable to water and slightly permeable to solutes
Na+ diffuses from the filtrate along their concentration gradient and move into nearby capillaries See Fig. 10.8B pg. 452 at the thick-walled part of the ascending loop of Henle, Na+ are moved out of the filtrate by active transport See Fig. 10.8C pg. 452 this transport of Na+ contributes to the salty environment of the medulla, and it makes the filtrate less concentrated compared to the tissues and blood vessels in the surrounding cortex, which is where the filtrate has now moved by now, about 65% of the Na+ and water from the filtrate has been reabsorbed
reabsorption of water and ions continues in the distal convoluted tubule (dct) passive reabsorption of negative ions, including Cl- also occurs by electrical attraction ion reabsorption continues to decrease the concentration of the filtrate, which water to continue to be reabsorbed by osmosis See Fig. 10.9 pg. 453
3. Tubular secretion moves additional wastes and excess substances from the blood into the filtrate ”fine-tuning” occurs here K+ are actively secreted from the bloodstream into the dct H+ are also actively secreted from blood into the dct, to maintain blood pH other substances that are not normally part of the body, including penicillin and other medications, are secreted from the blood into the dct reabsorption and secretion in the dct are under hormonal control
4. Water reabsorption collecting duct enters the medulla, which is a salty environment water is reabsorbed from the collecting duct by osmosis; increases the concentration of the filtrate if one is dehydrated (blood plasma is too concentrated) the distal tubule and collecting duct become more permeable to water, which causes more water to be reabsorbed and urine to be more concentrated; water is conserved
this process is under the control of the hormone ADH (anti-diuretic hormone) urea, uric acid, salts and other substances remain in the urine, which is now about 1% of the original filtrate volume Read pg. 449-454. Answer # 2-7, 10-12 pg. 455.