Download
1 / 61
650 likes | 1.11k Views
CT Anatomy and Pathology of the Urinary System, Adrenal Glands and Prostate. By Erik Poyourow MS3. First, some basic CT Principles you will need for this learning module. http://www.nowhow.nl/nederlands/images/CT-scanner.jpg. CT Basics.

E N D
CT Anatomy and Pathology of the Urinary System, Adrenal Glands and Prostate. By Erik Poyourow MS3
First, some basic CT Principles you will need for this learning module. http://www.nowhow.nl/nederlands/images/CT-scanner.jpg
CT Basics View the image is as if you were looking up from the patient’s feet. Right Left http://www.babalublog.com/archives/ToeTag.jpg
CT Basics > > > > Metal Bone Water Fat Air (tissue and blood) +500 to +1000 HU +300 to -500 HU 0 HU 0 to -50 HU -200 to -1000 HU • Things appear whiter according to their relative densities. • This property is called “Attenuation” and it is quantified in Hounsfield Units (HU), which can be measured on CT viewing software.
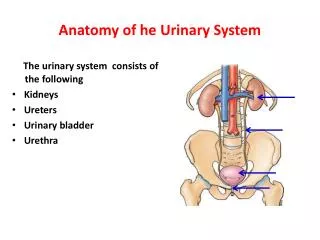
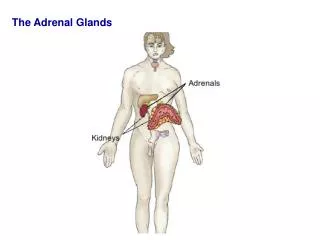
ADRENAL GLANDS • Adrenal glands • Located superior and medial to the kidneys and lateral to the diaphragmatic crura. • Like the kidneys they are within the Renal fascia and are therefore… • Surrounded by perirenal fat which appears dark on CT.
Adrenal glands They look like a “V” or a “Y” on CT. The Right Adrenal Gland is behind the IVC and medial to the liver. The Left Adrenal is lateral to the Aorta or Left Crus and posterior to the splenic vessels. Left click for answers. Identify the adrenals and associated structures. Aorta Right Hepatic Lobe Pancreas IVC Left Adrenal Right Adrenal Right Crus Left Crus
Kidneys Identify the following… Renal Artery and Vein *usually arise at L2 Capsule Pelvis Major Calyx Cortex Ureter Medulla Minor Calyx http://www.adam-rouilly.co.uk/products/Somso/MU3.jpg
Now Back to CT Anatomy Head of Pancreas Aorta IVC Superior Pole of Left Kidney comes into view first…
The Right Kidney comes into view a little more inferiorly… Watch the veins enter the IVC… …watch the arteries exit the Aorta. SMA IVC Left Renal Vein *entering the IVC, Left Renal Artery Superior Pole of Right Kidney Aorta Right Renal Artery *exiting the aorta
Following the vasculature down… SMA Left Renal Vein (*between SMA and Aorta) Right Renal Artery Left Renal Artery
Following the vasculature down… Left Renal Vein Right Renal Vein *coming off IVC Left Renal Pelvis *dives down wheras vessels run more horizontal Right Renal Artery Left Renal Artery
Following the vasculature down… Right Renal Vein Left Renal Vein Right Renal Artery Left Renal Artery
Following the vasculature down… Right Renal Vein Left Renal Vein
Fascial Compartments Anterior Renal Fascia (“Gerota’s fascia”) Look very closely! Note: this is the “Paraconal fascia” continuing anteriorly. Posterior Renal Fascia (“Zuckerkandl’s Fascia”) (Faint line) The Renal fascia divides perinephric (around the kidneys) from paranephric space (around the renal fascia). This becomes important when edema, pus or blood enters a compartment.
Phases of IV Contrast Depending on the timing, different structures are enhanced by IV contrast. • Pre-contrast Phase = Non-contrast – no enhancement. • Arterial Phase (15-25 seconds) • Angionephric or Venous Phase (30-60 seconds) The Renal cortex appears enhanced. • Nephrographic Phase (75-100 seconds) Cortex and Medulla appear enhanced. • Excretory/Urographic Phase (after 3 minutes -- routinely taken at 10 minutes) The collecting system is enhanced.
Anatomy of the Collecting System http://neosavina.ivyro.net/image/anatomy/adam/abdomen/aa51_1.gif
Post Contrast Image (Remember, it helps to visualize the Urinary Collecting System.) Pelvis Calyces
Structures related to the ureters IVC Aorta Right Ureter Left Ureter Psoas Muscles
Follow the Ureters Down along the Psoas Muscle Left Ureter Right Ureter Left Common Iliac Artery Right Common Iliac Artery Common Iliac Veins
After crossing over the branch point of the Iliacs, the ureters move along the lateral pelvic wall within the ureteric fold… Ureters
On their way to the bladder… Bladder
Finally the ureters enter the bladder posterolaterally. Bladder *dense contrast settles in the dependent bladder, with the urine on top. Ureters
What gender is this patient? What’s this below the Bladder, And anterior to the rectum? Prostate Strong work! In the next section try to use your understanding of CT anatomy to identify pathology.
Search Pattern • Adrenal Glands – limbs ≤ 1 cm thick, uniform, homogenous, and without convexities. • Kidneys – without enlargement, atrophy, distortion, striation, cysts or masses. • Fascial Compartments – without swelling, fluid, air or fat stranding • Pelvises and ureters – without dilation or obstruction. • Bladder – distension, wall thickness and contents in the lumen. • Prostate – without enlargement or nodules • Always be systematic in how you look at images. • Look for what is there and what is absent. • Don’t stop once you have found one thing wrong.
Urinary CT Pathology • The following slides show common CT findings. • Figure out what kind of image, is there contrast and if so where. • Identify the abnormality. • Then create a short differential in your head. By the way, what is the abnormality in this CT image? • Horseshoe Kidney congenital fusion 1-4/1000. • 3-4 x risk of Transitional Cell Carcinoma.
What is this? CASE #1 Foley bulb catheter in the bladder. Why is he catheterized? Left click to scan inferiorly and see if there is an obvious reason…
What is the abnormality? Does the pubis symphysis look wide to you? Hint: don’t forget to look at bones. Bladder And what’s herniating out between the pubic bones?
Pelvic Symphysis Diastasis http://www.swsahs.nsw.gov.au/livtrauma/education/sudden/pics/pelvis1.jpg • In pelvic fracture or diastasis, look for traumatic disruption of the urethra and bladder.
CASE #2 Does this person have 2 Gall Bladders? Where is the abnormality? Unlikely… so lets keep scanning down the body.
Hmmmm… that looks big. Left Click to keep scanning down…
Right Kidney What structure is involved? Based on the signal intensity what is the likely density of this lesion? Water.
Does it communicate with the vasculature? No, it is not contrast enhancing. Simple Renal Cyst (water), Hemorrhagic cyst (blood), Abscess (pus). Give a short differential.
Simple Renal Cyst • Very common “incidentaloma” in older patients (>50% in patients over 55 years old). • Smooth, thin walled cysts, without septae, that are homogenous near-water density (-10 to +20 HU) and non-enhancing are benign. • Smaller cysts may show “pseudoenhancement,” up to +10 HU due to various artifacts. • Usually asymptomatic and require no treatment. http://medlib.med.utah.edu/WebPath/jpeg1/RENAL002.jpg
What is the abnormality? CASE #3 Is this lesion involving other structures around it? What do you expect the Right Kidney to look like? Cortical Thinning + dilated renal pelvis = Hydronephrosis Yes, the Right Ureter is dilated. Thickened bladder wall. What is the differential? Transitional Cell Carcinoma, Squamous cell carcinoma. [Chronic cystitis, a trabeculated bladder or a nondistended bladder may show uniform thickening of the bladder wall.]
Transitional Cell Carcinoma http://www.pathology.vcu.edu/education/renal/images/dc.15.jpg • Typical Hx – Smoker, over 50 years old, with hematuria • 90% in bladder, but can arise all along the collecting system.
CT Basics Artifacts: things that mess up your image. • Patient Motion • Volume Averaging – the computer averages the density of a cubic unit called a “voxel,” and attributes a brightness to it. So depending on what is around the structure of interest it can appear more or less dense on CT. • Beam Hardening – “streaks” appear because low energy photons are absorbed by high density material (metal, bone, etc.).
Where is the abnormality? CASE #4 Left click to magnify the image.
Do you see any “beam hardening”? So, what “attenuation” (density) are these? Metal What disease is this person being treated for? Prostate Cancer. (These are radioactive seeds implanted in the prostate, “Brachytherapy.”)
Prostate Cancer • #1 Cancer diagnosis in men. • Extremely common in older men. • Brachytherapy uses radioactive seeds placed inside the prostate. http://encyclopedia.quickseek.com/images/Brachytherapy.jpg http://www-medlib.med.utah.edu/WebPath/jpeg1/MALE074.jpg
Do you see an abnormality? CASE #5 How about if we add some IV contrast?
Can you identify the abnormality now? Does it enhance with contrast? Lets look at both images side-by-side.
Is this lesion enhancing or non-enhancing? Enhancing! Even if you couldn’t see the contrast in the lesion, you could check the HU to be sure. Is this arising in the cortex or medulla? Cortex What is your differential? Renal Cell Carcinoma
Renal Cell Carcinoma (RCC) • 90% solid kidney tumors • Arises in the cortex from the Tubules • Generally enhance 10-25 HU with IV contrast due to hypervascularity. • 5% cystic (septae, thick walls), especially as they enlarge but still enhance with contrast. http://pathology.catholic.ac.kr/pathology/specimen/kidney/sp-36.jpg
Where is the abnormality? CASE #6 What Structure is it involving? Right Adrenal Gland