Download
1 / 10
120 likes | 402 Views
Diabetic Nephropathy. Rick Allen. Definition. a glomerulonephropathy is defined by characteristic structural and functional changes Structural : mesangial expansion, GBM thickening and glomelular sclerosis. Functional : hyperfiltration and albuminuria. Epidemiology.

E N D
Diabetic Nephropathy Rick Allen
Definition • a glomerulonephropathy is defined by characteristic structural and functional changes • Structural: mesangial expansion, GBM thickening and glomelularsclerosis. • Functional: hyperfiltration and albuminuria.
Epidemiology • DM type I – 20-30% develop microalbuminuria after 15 years. <1/2 of these overt nephropathy. Can regress or remain stable. Now dropping due to effective control methods. • DM type II – As above? Rates on the rise due to increased fatty numbers. • Leading cause of premature death in young diabetics. Second to MI overall.
Risk Factors • Type I = Type II (we think. Start time dubious) • GENETICS (AT2, ACE) • HTN • High GFR • Poor hyperglycaemic control (high HbA1c) • Obesity • Smoking • OCP • Race (blacks 3-6x > whites)…SES? + above. • Age…unknown, however DM I Dx <5y.o. is good
Ix • earliest detectable sign is microalbuminuria. • Macroalbominuriais more predictive for future developmet of severe nephropathy and decreased GFR.
Pathophysiology and Pathology • Glomerular sclerosis/damage • Metabolic defect; insulin deficiency hyperglycaemia biochemical alterations in GBM (increased collagen type IV and fibronectin, decreased proteoglycan) and increased ROS ( damage) • Nonenzymatic glycosylation inflammatory cytokines and GF released from macrophages, ROs generation in endothelial cells, increased procoagulant activity in endothelial cells and macrophages, ECM synthesis and SM prolif. • Haemodynamic changes increased GFR, glomerular capillary pressure, glomerular filtration area, and glomerular hypertrophy. • Afferent arteriole is damaged bigger afferent than efferent increased GFR and pressure, causing further damage and increased shearing forces mesangial cell hypertrophy and excretion of ECM products glomerular sclerosis
Pathophysiology and Pathology 2 • Ischaemia (due to hypertrophy of afferent and efferent arterioles) • hypertrophy and hylanization of vessels ischaemic kidney damage • Ascending infection • Occur more in women with diabetes than without. No difference for men. Causes: bladder stasis (neuropathy), infections like to live in damaged kidney (easier to get established)
Pathophysiology and Pathology 3 • Under the microscope we get • Glomerular lesions: GBM thickening, diffuse mesangial sclerosis (PAS positive for stain) and nodular glomerulosclerosis (Kimmelstiel-Wilson lesion, + hyaline accumulations in fibrin caps [in capillary loops] and capsular drops [adhere to Bowman’s capsule]. 15-30% of long term diabetics get this, most associated with renal failure.) • Vascular lesions: arteriosclerosis/hylanisation of afferent and efferent arterioles • Pyelonephritis, including necrotising papillitis. • Glomerular and vascular lesions ischaemia tubular atrophy and interstitial fibrosis overall contraction in size.
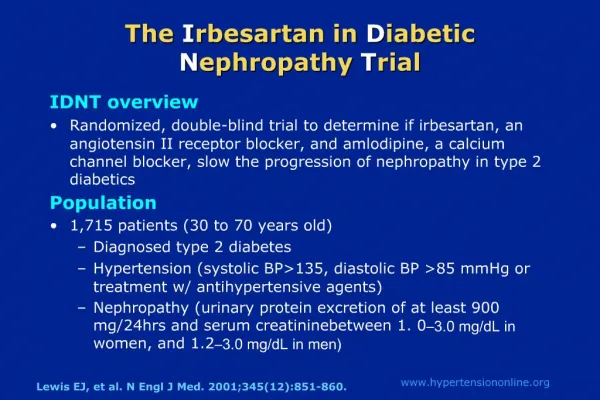
Tx and management • Same as any other chronic renal disease, however; • Use an ACEI or AT2 inhibitor to get that BP down! • Avoid oral hypoglycaemics excreted by the kidney (metformin) • Assess insulin dose and effectiveness • Retinopathy may cause issues with treatment (blind, can’t see what doing) • Haemodialysis may be difficult as fistulas calcify rapidly. Peritoneal. • Kidney transplant failure is higher than pt. without DM.