Diabetic nephropathy
Diabetic nephropathy. Diabetic nephropathy- definition. Chronic microangiopathy type complication of DM characterized by: proteinuria hypertension p rogressive loss of GFR leading to ESRD. Microalbuminuria. albumin excretion in urine 30 – 300 mg/d or 20 – 200 ug/min


Diabetic nephropathy
E N D
Presentation Transcript
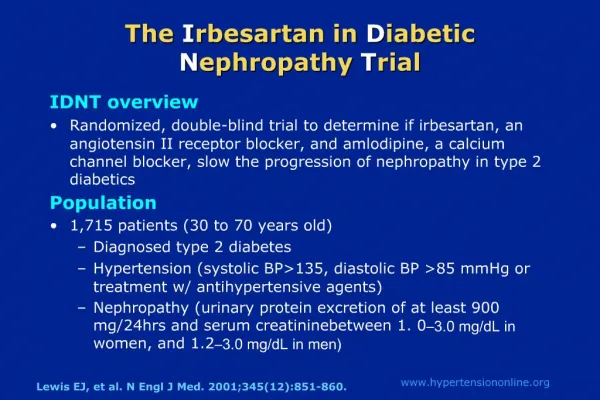
Diabetic nephropathy- definition Chronic microangiopathy type complication of DM characterized by: proteinuria hypertension progressive loss of GFR leading to ESRD
Microalbuminuria • albumin excretion in urine 30 – 300 mg/d or 20 – 200 ug/min 2. If temporary, but >80 mg/d it means in 95% progression to continuous microalbuminuria 3. If continuous - it means threatening nephropathy. Not treated increases 20 – 40% a year. After 5 years becomes macroalbuminuria= evident diabetic nephropathy
Macroalbuminuria • Albumin excretion in urine >300 mg/d 2. It may lead to development of nephrotic syndrome (proteinuria, hypoalbuminaemia, hyperlipidaemia, edema) 3. ESRD appears usually after 5 years
Time course of DN according to type of DM (Mogensen scale) IDDM NIDDM I stadium (0-2 yrs) hyperfiltration (100%) (unnoticeable) II stadium (2-5yrs) silent DN (100%) (100%) III stadium (>5 yrs) threatening DN (30%) (30%) IV stadium (>15 yrs) evident DN (25%) (25%) V stadium (>15 yrs) ESRD (20%) (20%)
Factors contributing to development of DN • Long-lasting hyperglycemia • Family predisposition • HT • High-protein diet • Cigarette smoking • hyperlipidaemia
BP in children of DM patients without DN with DN SBP 117 +13 mmHg 125 +17 mmHg Strojek i wsp. Mutual coincidence of DM and HT
DM patients with HT • Age of DM patients = % of patients with HT
Treatment of DN • Proper treatment of DM • Proper treatment of HT • Quit smoking habit • Control of protein content in diet • Early treatment of anaemia • Early kidney replacement therapy
Proper treatment of DM • „Almost normal” glycaemia: fasting 60 – 140 mg/dl 2 h after meal <200 mg/dl • Proper body mass • Correction of hyperlipidaemia
Proper treatment of BP • Lowest tolerable BP • Treatement with ACE-I & AT-II
Nutrition state (albuminaemia) and the risk of death Hakim 1994
Early treatment of anaemia with epo Anaemia… when? glomerulonephritis DN GFR <25-30 ml/min<35-40 ml/min creatinine >3-4 mg/dl >2-3 mg/dl Attention: ACE-I may contribute to anaemia!
Early start of renal replacement therapy • creatinine >3,5 – 4 mg/dl – a-v fistula! • creatinine >4,5 – 5 mg/dl (GFR <20 ml/min): - consider KTx (<45 yrs & IDDM) - consider KTx and pancreas Tx (>45 yrs & NIDDM) - start RRT
HD therapy in DM patients Pro: Contra: High efficiacy CVS damage Frequent control problems with a-v fistula No protein loss Hypotonia frequent hypoglycaemia frequent hyperkalaemia
CADO treatment in DM patients Pro: Contra: CVS neutral risk of infection No a-v protein loss Good control of kalaemia hernias Good control of glycaemia helper required
Glycaemia regulation in DM patients with ESRD • Gluconeogenesis decreased by 30 – 40% • Insulin requirement decreased 3-4x 3.Decreased metabolism of some oral drugs (eg. metformin) • During HD glucose is „hemodialysed” and lost All the above may lead to hypoglycaemia!
DM patient on HD therapy- what should be the treatment? • Insulin – 2-3x lower doses! • Oral drugs – short acting, metabolized in liver eg: - glipizyd (Glipizyd, Minidiab, Glibenese GITS) - gliclazyd (Diaprel, Diabezyd) - glikwidon (Glurenorm)