Download
1 / 34
370 likes | 699 Views
Pelvic Floor Prolapse. M L Padwick MD FRCOG. IN THE NAME OF GOD. What is prolapse ?.

E N D
Pelvic Floor Prolapse M L Padwick MD FRCOG
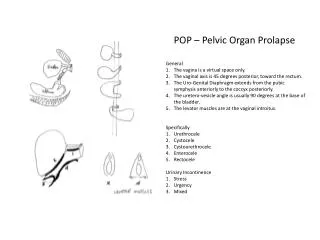
What is prolapse ? • Prolapse is a condition in which organs, which are normally supported by the pelvic floor, namely the bladder, bowel and uterus, herniate or protrude into the vagina. This occurs as a result of damage to the muscles and ligaments making up the pelvic floor support. At least half of women who have children will experience prolapse in later life.
Statistics • ratio surgery for prolapse vs incontinence: 2:1 • prevalence of 31% in women aged 29-59 yrs • 20% of women on gynaecology waiting lists • 11% lifetime risk of at least one operation • re-operation in 30% of cases
Factors associated with pelvic floor prolapse • age • parity • big babies • menopause • obesity • occupation • home delivery • family history
Diagnostic Approach • fig4
Pathophysiology • Table 1
Pathogenesis • childbirth • connective tissue disorders • menopause • chronic intra-abdominal pressure • iatrogenic (hysterectomy)
What are the symptoms of pelvic floor prolapse? • This depends on the types and the severity of the prolapse. • Generally, most women are not aware of the presence of mild prolapse. • When prolapse is moderate or severe, symptoms may include sensation of a lump inside the vagina or disturbance in the function of the affected organs, such as:
Bladder • stress incontinence • urgency • frequency • incomplete emptying • dribbling • recurrent urine infections
Bowel • low back pain or discomfort • incomplete emptying • constipation • manual decompression • incontinence of flatus
Sexual problems • looseness and lack of sensation • difficult entry and expulsion • discomfort or painful intercourse • vaginal bleeding in neglected cases
Other • can see and feel it • back ache • dragging sensation • increased discharge • skin irritation
How can prolapse be prevented? • appropriate antenatal and intrapartum care • regular postnatal pelvic floor exercises to compensate for childbirth damage • in postmenopausal women, oestrogen cream helps maintain tissue strength
Living with pelvic organ prolapse Avoid standing for long periods of time. Do pelvic floor exercises Prevent or correct constipation Wear a girdle Try yoga Wear a pantyliner or incontinence pad Explore alternatives to sexual intercourse Carry wet wipes
Pelvic organ prolapse Non-surgical treatments • Physiotherapy - pelvic floor exercises and • Hormone Replacement Therapy (HRT) - may be local oestragens • Vaginal Pessaries - many choices but regular checks and changes needed and best combined with oestragen creams
Genital prolapse and Pelvic floor muscle exercises Summary We found no RCTs or observational studies of sufficient quality examining the effects of pelvic floor muscle exercises on the symptoms of genital prolapse. Comment Although pelvic floor muscle exercises appear to be effective in reducing the symptoms of urinary stress incontinence (see benefits of pelvic floor muscle exercises in stress incontinence chapter), their usefulness in the treatment of genital prolapse is unproven.
Nutrititon. Supplements The supplement programme below should be taken for at least three months in order to achieve best results Your supplement plan — A good multivitamin and mineral tablet — Vitamin C with bioflavonoids (1000mg twice a day) — Vitamin A (as beta-carotene at 25,000iu per day) — Proanthocyanidins (50 mg per day) — Manganese (5mg per day) — Cranberry supplement (only needed for stress incontinence) At the end of three months you should reassess your condition and adjust your supplement programme accordingly.
The Surgical Management of Prolapses • Restoration of pelvic structures to normal anatomical relationship • Restore and maintain urinary &/or faecal continence • Maintain coital function • Correct co-existing pelvic pathology • Obtain a durable result Principles of Pelvic Reconstructive Surgery
The Surgical Management of Prolapses Patient assessment • Careful history • Physical examination • Neurological assessment • Urodynamic evaluation • Anorectal investigations
The Surgical Management of Prolapses Factors affecting choice of operation • Surgeons' own expertise, experience and preference • Pre-op voiding or bowel dysfunction • Duration of efficacy • Complications • Learning curveof life factors • First or repeat surgery • The need to treat other pathology • Fitness of the patient • Underlying pathology • Success rates for different procedures
The Surgical Management of Prolapses • Uterovaginal prolapse is multifactorial in origin • Treatment needs to be individualised • Approach often needs to be multidisciplinary • Quality of life assessment is essential Summary - Female Pelvic Organ Prolapse
Types Of Surgery • Anterior and posterior repairs • Vaginal hysterectomy • Laparoscopic vaginal vault suspension (± mesh) • Laparoscopic sacrocolpopexy • Laser Vaginal Rejuvenation • Designer Laser Vaginoplasty • Vaginal approach to prolapse repair incorporating mesh • Laparoscopic paravaginal repairs
Total colpocleisis procedure often coupled with a tension free vaginal tape (TVT) sling procedure for urinary incontinence
Sacrocolpopexy and paravaginal repair for total pelvic floor prolapse