Download
1 / 44
480 likes | 1.31k Views
Wrist and Hand Anatomy and Injuries. Morgan Scott, MS, ATC, LAT. Unit Objectives. Understand the basic anatomy of the wrist and hand Explain various types of injuries that occur Understand the common mechanisms of injury Understand the signs and symptoms of the various types of injuries.

E N D
Wrist and Hand Anatomy and Injuries Morgan Scott, MS, ATC, LAT
Unit Objectives • Understand the basic anatomy of the wrist and hand • Explain various types of injuries that occur • Understand the common mechanisms of injury • Understand the signs and symptoms of the various types of injuries
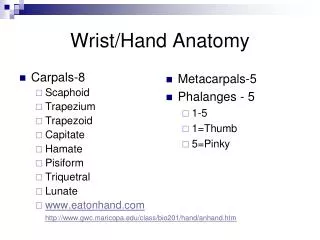
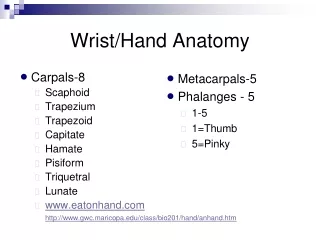
Carpal Bones • Pneumonic for carpal bones Of the wrist • Some (Scaphoid) • Late (Lunate) • Trainers (Triquetrium) • Practically (Pisiform) • Taped (trapezium) • Tommy’s (trapezoid) • Clean (Capitate) • Hand (Hamate)
Metacarpals & Phalanges • There are 5 metacarpal bones (numbered I-V, starting with the Thumb) • There are 14 Phalange Bones • The thumb is the only finger with 2 phalanges
Wrist and Hand Joints • The Carpometacarpal Joint is located where the carpal bones meet the metacarpals (hand) • The Metacarpal phalangeal joint is located between the hand and the fingers • The Interphalangeal Joints are between each phalange (if you look at your fingers, everywhere you have creases, there is a joint)
Wrist Muscle Anatomy • The wrist and hand movements are controlled by many different muscles. • The flexor muscle groups are located on the anterior surface of the forearm. • The extensor muscle groups are located on the posterior aspect of the forearm.
Wrist Ligaments • Most injuries to the wrist and fingers are sprains. • Of major interest in wrist injuries are: • Ulnar Collateral Ligament: extends from ulna to the pisiform • Radial Collateral Ligament: extends from the radius to the scaphoid • Transverse Carpal Ligament: crosses the volar aspect of the carpal bones • One common misconception about sprains of the fingers is that they must be pulled back into place. This is NOT true!
Phalangeal Joints • Each phalangeal joint has an articular capsule that is reinforced by collateral and volar ligaments. • The interphalangeal joints are of hinge type, permitting only flexion and extension. • Distal Interphalangeal • Proximal Interphalangeal (closer to wrist)
Neurovascular Supply • Ulnar Nerve: little finger, sensory to dorsal, digits 4-5 • Median Nerve: volar hand and fingers, thumb opposition, finger flexors • Radial Nerve: Dorsum of hand, extensor muscles
Palpations • Scaphoid • Trapezoid • Trapezium • Lunate • Capitate • Triquetrium (triquetral) • Pisiform • Hamate • Metacarpals • Proximal phalanges of the fingers • Middle phalanges of the fingers • Distal phalanges of the fingers • Proximal phalange of the thumb • Distal phalange of the thumb • Ulnar Collateral Ligament of the wrist • Radial collateral Ligament of the wrist
Preventing Wrist Injuries • Protective equipment can be used to prevent injury. Some items include; • Braces • Tape • Gloves • Padding • Be aware of the rules of the sport. Some sports prohibit the use of hard substances such as braces or only allow protective equipment with a doctors note.
Evaluation of Hand and Wrist Injuries • History: Ask questions? • General Inspection • Posturing of the hand • Gross deformity • Palmar creases • Areas of cuts of scars • Inspection of Hand and wrist
Wrist/ Forearm Fractures • Fractures of the forearm are common in children and youths. • Etiology: direct blow or fall on outstretched hand. • Direct blow to forearm usually results in ulna fracture. • Signs and symptoms: audible crack, pain, swelling disability. • Management: RICE, Splinting, Refer to doctor.
Colles’ Fracture • Most common types of forearm fractures. • Involve lower end of radius or ulna. • Mechanism: FOOSH • Less common is the reverse of Colles’ Fracture; Mechanism is fall on back of hand. • S/S: forward displacement/ visible deformity (silver fork deformity) • Management: Cold compress, spilint, sling, refer for X-rays. • No complications: athlete will return in 1-2 months
Wrist Sprains • Most common wrist injury which occurs from overuse, falls, and forceful twisting motion. • Signs and symptoms: Pain, decreased ROM, decreased grip strength, swelling • Management: RICE, Reestablish ROM and strength, Tape or brace on return to activity for support • ** The main support for the wrist is derived from posterior and anterior ligament which transport vessels to the carpal bones and stabilize the joint. • Therefore, repeated sprains may disrupt circulation.
Critical Thinking • An athlete who sustained a major wrist sprain complains of a decrease in hand circulation. • How should this injury be evaluated for a circulation problem?
Allen’s Test • Allen’s test is used to determine the function of the radial and ulnar arteries supplying the hand. • The athlete is instructed to open and close the hand in a tight fist 3 or 4 times. • While the athlete is holding the last fist, the ATC places firm pressure over each artery. • The athlete is instructed to open their hand. The palm will be a white color. • One artery is then released, if normal the hand will become instantly red.
Triangular Fibrocartilage Complex Injury (TFCC) • The TFCC is a fibrous structure that seperates the radiocarpal and radioulnar joints in the wrist. • It is the major ligamentous stabilizer of the distal radioulnar joint. • The TFCC functions like the meniscus of the knee. • It is prone to cartilage tears that could cause wrist pain and clicking. Similar to meniscus tears.
Triangular Fibrocartilage Complex Injury (TFCC) • Etiology: forced hyperextension of the wrist which compresses the TFCC between the radioulnar joint and carpal bones. • S/S: It is common for an athlete to not report this injury immediately. Pain along ulnar side of wrist, clicking or catching, swelling. • Management: refer to Doctor. • Immobilized for 4 weeks
Carpal Tunnel Syndrome • Located on anterior aspect of wrist. • Floor: carpal bones • Roof: transverse carpal ligament • Many structures go through this space, such as: • 8 finger flexor tendons, median nerve • Etiology: results from inflammation of tendons and synovial sheaths which ultimately leads to compression of median nerve. • Repeated wrist flexion or direct trauma
Carpal Tunnel Syndrome • S/S: Compression of median nerve will result in both sensory and motor defecits. • Sensory changes: tingling, numbness, and paresthesia over the thumb, index and middle fingers and palm of hand. • Motor changes: weakness in thumb movement • Management: RICE, immobilize and NSAIDs. If condition persists injection with corticosteriod and possible decompression of the transverse carpal ligament
Critical Thinking • A shot-putter is beginning to feel tingling, numbness, and paresthesia in the thumb, index, and middle fingers and palm of right hand. • The athlete is demonstrating a carpal tunnel syndrome. What factors could produce this problem?
Dislocation of the lunate bone • Dislocations are infrequent in the wrist during athletic competition. • The lunate bone is the most commonly dislocated. • Mechanism: Forceful hyperextension, FOOSH. • The lunate is usually dislocated anteriorly. • S/S: Pain, swelling, and difficulty flexing wrist and fingers • Management: Refer to doctor, if not detected early enough, bone deterioration may occur.
Scaphoid Fracture • Most frequently fractured of the carpal bones. • Mechanism: FOOSH which compresses the scaphoid bone between the radius and second row of carpal bones. • Without proper splinting, the fracture often fails to heal because of an inadequate supply of blood, thus degeneration and necrosis occur. • S/S: Swelling in area of carpal bones, severe point tenderness in anatomical snuff box.
Scaphoid Fracture • Management: apply cold and splint, refer for x-ray. Immobilization usually takes place for 6 weeks and is followed by strengthening. The wrist also need protection against impact loading for 3 months.
Hamate Fracture • Mechanism: FOOSH but more commonly from contact while the athlete is holding a tennis racket, baseball bat, lacrosse stick, hockey stick or golf club. • S/S: wrist pain, weakness, and point tenderness. • Management: Casting. The hook of the hamate can be protected by a donut shaped pad to take the pressure off the area.
Wrist Ganglion • Wrist ganglion is a synovial cyst which is considered to be a herniation of the joint capsule or synovial sheath. • S/S: occasional pain with lump at the site. May feel soft, rubbery or very hard. • Management: Aspiration or digital pressure and pressure pad. Ultrasound can be used to reduce the size of the cyst.
Critical Thinking • A soccer player falls on the outstretched left hand, causing a compression force to the scaphoid bone between the radius and second row of the carpal bones. • What wrist injury is most likely to have occurred?
Group work • Get into 3 groups. • Pick a wrist injury • Draw wrist/ Hand on poster. • Emphasize area of injury • Write on poster: Mechanism, Signs and Symptoms, Management.
Trigger Finger • Etiology: Inflammation of the tendon sheath which leads to swelling, crepitis, and painful movement. • Most commonly affected are the extensor tendons. • S/S: Complains that when the finger or thumb is flexed, there is resistance to reextension; which produces snapping. • Management: Corticosteriod and splinting.
Mallet Finger • Sometimes called baseball finger or basketball finger. • Etiology: Caused by blow from a thrown ball that strikes tip of finger; jamming and avulsing the extensor tendon. • S/S: Pain at DIP joint, athlete unable to extend the finger, carrying it at a 30 degree angle. • Management: RICE, if not fractured, the distal phalanx should be splinted immediately in extension.
Boutonniere Deformity • Etiology: The boutonniere or buttonhole deformity is caused by a rupture of the extensor tendon to the middle phalanx. Trauma occurs to tip of finger which forces the DIP joint into extension and PIP joint into flexion. • S/S: Severe Pain and inability to extend DIP joint, swelling, obvious deformity. • Management: Cold application followed by splinting.
Jersey Finger • Etiology: Rupture of the flexor tendon from its insertion on the distal phalanx. • This condition most often occurs on ring finger. • S/S: The tendon is no longer attached to the distal phalanx, the DIP joint cannot be flexed. • Management: If the tendon is not repaired surgically, the athlete will never be able to flex the DIP, causing grip weakness.
Critical Thinking • A baseball catcher receives a pitch that jams and avulses the extensor tendon of the DIP joint of the second finger. • How should this condition be managed?
Wrist & Finger Review Questions • Describe the Colles’ fracture of the forearm—Cause, appearance, care. • Describe the mechanism, symptoms, and signs of a wrist sprain. • What healing problems occur with a scaphoid fracture? • Describe the circumstances that can produce a mallet finger and boutonniere deformity in baseball players. What care should each condition be given?