Download

1 / 57
570 likes | 769 Views
STAFF CONFERENCE: 11 year old Sickler with Fever. Renee Thompson M.D. CASE ID. KK 11 year old female From St. Thomas (U.S. Virgin islands) Known to have HbSC disease. HISTORY. Presented to the Roy L. Schneider hospital on 5/9/10 with a 7 day history of intermittent mild fevers (subjective)

E N D
STAFF CONFERENCE:11 year old Sickler with Fever Renee Thompson M.D.
CASE ID • KK • 11 year old female • From St. Thomas (U.S. Virgin islands) • Known to have HbSC disease
HISTORY • Presented to the Roy L. Schneider hospital on 5/9/10 with a 7 day history of intermittent mild fevers (subjective) • Generalized abdominal pain- intermittent and cramping in nature (LMP 5/3/10) • Diarrhea – 3-4 episodes of watery non-bloody stools per day, no mucus in stools • Headache
HISTORY • Weakness which progressed into lethargy on the day prior to presentation • Loss of appetite • No cough or URI symptoms • No urinary symptoms • No vomiting • No retroorbital pain • No hematuria or nosebleeds or easy bruising • No ill contacts at home
HISTORY • PMH: • HbSC disease, admitted 3 times in the past, twice for VOC and once for pneumonia. • No h/o ACS, intubation, splenic sequestration, transfusion, gallstones • PSH: nil • Medications: Folic acid daily • Allergies: nil • SH: Lived with father in St. Thomas, moved from Dominica 3 years ago, mother still resides there • Immunization: UTD • FH: Mother HbAC, Father HbAS, no other FH of sickle cell disease, siblings only have sickle cell trait
PHYSICAL (RLS) – 5/9/10 0800 • Ill-looking but alert female in mild respiratory distress. MM pale and moist. Icteric, acyanotic • T 38.2 • Chest clear • Abdomen soft and mildly tender over spleen which was palpated 6 cm below LCM, no hepatomegaly, good BS • Neuro: no deficits • CVS: S1 and S2 heard normally with no murmurs or other additional heart sounds, good perfusion throughout
LABS – RLS 5/9/10 0800 • Hb 8.3 (baseline 12) • Wbc 17.9 • PLT 12 • PT 21 PTT 32 INR 2.5 • Na 129 K 6.9 (not hemolysed), BUN and Creatinine were normal at that time
LABS – RLS 5/9/10 1800 • Hb 4 • wbc 59.8 • PLT 10 • BUN 23 • Creat 2.4
HOSPITAL COURSE (RLS) • After BUN and Creat were noted to be elevated, KK received a 2L bolus of N/S then was placed on D5NS at 100 ml/h • Ceftriaxone, Vancomycin and Zithromax were started • Transferred to the ICU, left femoral line placed • Transfused with FFP and PRBC • CT of Abdomen: possible ischemia of the bowel, bilateral renal cortical necrosis, right pleural effusion, pneumonia, moderate fluid in pelvis and Abdomen
HOSPITAL COURSE (RLS) • Within a few hours she became hypoglycemic • Worsening renal function with persistent hyperkalemia • Mixed acidosis • Worsening coagulopathy with increasing PT, PTT and INR of 30 • Increasing liver enzymes • At the hospital attempts were made to correct these derangements with transfusions, IVF and Calcium Carbonate but she continued to deteriorate
HOSPITAL COURSE (RLS) • At 0310 on 5/10/10 she was intubated due to altered mental status and shallow breathing • Severe hypotension requiring pressor support with dopamine and eventually norepinephrine and epinephrine • Transferred to JMH PICU on 5/10/10, arrived at 1245 for further management
Examination - JMH • Sedated intubated female, icteric with pale MM • Vitals: T 35.8 HR 141 BP 155/93 CVP 14 ETCO2 33 RR 0 O2 sat 94% • HEENT: PERLA, Pupils 4mm • Resp: • Settings: Rate 20 Vt 500 PEEP 5 FiO2 60 • Air entry diminished bilaterally, Breath sounds coarse, no crackles, no wheezes
Examination-JMH • CVS: • S1 and S2 heard normally, no murmurs, no rubs or gallops • feet and hands cold to touch with weak radial and dorsalis pedis pulses. CR >3s • Femoral line noted to left groin, pressure bandage over right groin, blood noted to be oozing around all bandage sites • Abdomen: • Distended tense abdomen, Bladder Pressure 19, BS absent, no masses • Unable to palpate for spleen and liver due to tenseness of abdomen. • NG drainage- coffee ground, Urine cath drainage – minimal and bloody
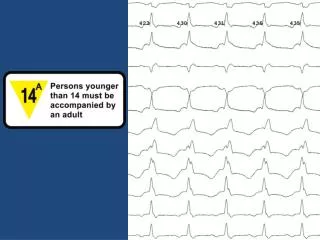
Admission Labs 7.18 / 51 / 25 / 18 / -10 7.4 89 26.1 PT 46.9 PTT 57.9 INR 4.11 Fib 41 19.7 N 53 L 21 M 11 Ca 9.8 P 12 Mg 2.6 Tpr 4.2 Alb 2.3 Tbili 4.6 Dbili 2.9 LDH >12900 AST >4500 ALT 4548 Alk P 158 GGTP 38 Amylase 809 Lipase >4000 Amm 75 Lactic A 21.7 141 93 17 185 5 24 2.88
Imaging • U/S 5/10/2010: • Gallbladder wall thickening, splenomegaly and ascites which in the appropriate clinical setting can be seen with dengue fever, but are nonspecific findings. • Bilateral echogenic kidneys likely on the basis of medical renal disease.
Assessment • 11 yo female with HbSC disease • Multiorgan failure most likely due to septic shock • Respiratory failure, liver failure, renal failure, circulatory collapse • Differentials for septic shock: • Bacteremia • Viremia • Hemorrhagic shock secondary to dengue fever • Right Pleural effusion • Abdominal compartment syndrome
PLAN • RESP • Continue ventilation and monitor gases every 4 hours to monitor and correct as needed the metabolic acidosis • Chest tube placed on right for Pleural effusion • CVS • Continue pressor support with Epinephrine, Norepinephrine, Dopamine and CaCl • Wean pressors as tolerated
PLAN • FEN/GI/RENAL • Keep NPO • Nexium IV bid for Ulcer prophylaxis • NG tube to low suction • D10W with bicarb infusion 50 ml/h • CVVHD started to improve electrolytes and fluid status • Peritoneal drain inserted and fluid sent for analysis and culture • HEME/ID • FFP, cryoprecipitate and Factor VII to be given in an attempt to control coagulopathy, monitor PT and PTT • Peritoneal and pleural fluid sent for culture • Blood, endotracheal aspirate and urine sent for culture (viral, mycology, bacterial)
PLAN • Heme/ID • Vancomycin, Flagyl and Ceftriaxone started empirically • Blood sent for Dengue PCR, Hepatitis panel • CBC followed closely and blood products to be transfused as needed • Neuro • Keep Sedated with Versed and Fentanyl • Paralyzed with Rocuronium • To be titrated as necessary • ID, Nephrology, Cardiology, Hematology, PDS and Transplant consults obtained
Day 1 Labs 7.26 / 59 / 71 / -1 9.1 171 28.7 PT 23 PTT 40.8 INR 2.02 Fib 174 25.5 N 62 L 6 M 4 Ca 13.5 P 12 Mg 2.6 Tpr 7.1 Alb 2.3 Tbili 10.4 Dbili 4.4 AST >4500 ALT 4396 Alk P 275 GGTP 90 Amm 12.7 Lactic A 15.5 149 101 12 72 4.5 26 2.17
Day 1 • FEN/GI/Renal • KK continued to have elevated bladder pressures (29) and ELAP was done by PDS at bedside. • No areas of nonviable intestinal necrosis or perforation. • Visualization of the liver showed a hemorrhagic degeneration of the liver with multiple petechiae and signs of ischemia. • Liver duplex: • Thrombosis of the right portal vein. Minimal flow seen in the mid portal vein concerning for impending thrombosis • Spleen also noted to be engorged and enlarged • Silo placed • Continued on CVVHD and when BP allowed 40 ml/h was removed • Still NPO
Day 1 • Resp • Patient continued to be intubated and required bicarb boluses for continued mixed acidosis • Due to fluid overload she had worsened pulmonary edema and this made it more difficult to ventilate her • She continued to require increasing FiO2s • Frequent adjustments were made to her vent settings (conv)
Day 1 • CVS: • Continued to require pressor support to maintain normal blood pressures • Heme/ID: • Continued antibiotics as no results back yet. No positive cultures • Required PRBC, PLT and FFP
Day 2-7 • Resp: • Continued deterioration with acidosis and CO2 retention. She was switched on Day 2 to HFOV. Chest tube drainage minimal but bloody and patient was too coagulopathic to pull tube • CVS: • Able to discontinue epinephrine but continued to require norepinephrine and dopamine to remain normotensive. At first she was thought to be intravascularly depleted but when Swan Ganz placed on Day 3 her CVP and wedge pressures did not suggest this
Day 2-7 • FEN/GI/Renal • Continued to be fluid overloaded, CVVHD had to be held at times as her BP was too labile. • Lasix drip to attempt diuresis • HAL was started by Day 2 • Silo output was in excess of 2L daily and was replaced with 5% Albumin • LFTS continued to be elevated but then by Day 3 started to trend downwards, thought to be due to burn out of the liver • Plasmapharesis was performed daily for 4 days • Creatinine remained consistently elevated in the 2s • Still anuric
PLASMAPHERESIS • Therapeutic plasma exchange (TPE, plasmapheresis) is an extracorporeal blood purification technique designed for the removal of large molecular weight substances from the plasma • Most commonly performed with centrifugation devices used in blood banking procedures. These offer the advantage of allowing selective cell removal (cytapheresis). However, an increasingly popular and often more efficient method of plasma separation is the use of a highly permeable filter with standard HD equipment • Requires reliable venous access, (either 2 large, durable peripheral veins, or a central line using a catheter which has a dual lumen and is rigid enough to withstand significant flow and pressures)
PLASMAPHERESIS • The fluid volume removed by TPE must be replaced to prevent marked volume depletion. • Albumin, alone or with saline, and FFP can be used. Each has advantages and disadvantages, and the optimal choice often varies with the clinical setting. We use albumin for most conditions, saline for hyperviscosity, some combination of albumin and saline if cost is a consideration, and FFP for TTP • Albumin solutions have the advantages of lack of viral transmission and minimal risk of anaphylactoid reactions. There is, however, a postpheresis depletion coagulopathy and a net loss of immunoglobulins • FFP replaces the normal proteins that have been removed. As a result, there is no depletion of coagulation factors or immunoglobulins. However, complications are more common than with albumin.
Indications for plasmapheresis • At least one of the following conditions must be present for TPE to be a rational therapeutic choice: • The substance to be removed should be sufficiently large (mol wt greater than 15,000) so that it cannot be easily removed by less expensive purification techniques such as hemofiltration or high-flux hemodialysis. • The substance to be removed must have a sufficiently long half-life, so that extracorporeal removal is much more rapid than endogenous clearance pathways. • The substance to be removed must be acutely toxic and resistant to conventional therapy, so that the rapid elimination from the extracellular fluid by TPE is indicated
Why did we do it? • Plasmapheresis is being used more commonly now in Intensive care units in patients with in septic shock and in those with multiorgan dysfunction • The premise is simple, if the plasma of the patient contains toxic materials (e.g. endotoxins, cytokines) then why not remove it and replace it with plasma with “good materials” (e.g. proteins in FFP) • References: • Plasma exchange in patients with septic shock including Acute Renal Failure Stegmayr BG Blood Purif. 1996;14(1):102-8. • Is there a role for plasmapheresis/plasma exchange therapy in septic shock, MODS, and thrombocytopenia-associated multiple organ failure? We still do not know--but perhaps we are closer. Carcillo JA, Kellum JA. Intensive Care Med. 2002 Oct;28(10):1373-5. • Utility of plasmapharesis in intensive care • Med Intesiva. 2010 Jan-Feb; 34(1): 74-8. • Salazar, Ramirez C, Daga Ruiz D, Cota Delgado F, Fernandez-Aquirre C, Fernandez Anno JM, Garcia Fernandez JM
Plasma Exchange Restores factor homeostasis as per plasma infusion In addition: Removes ADAMTS-13 inhibitors Removes ultra-large vWF multimers Removes tissue factor Removes excess PAI-1 Maintains fluid balance during procedure • Plasma Infusion • Restores procoagulant factors • Restores anticoagulant factors (protein C, AT III, TFP-I) • Restores prostacyclin • Restores tPA • Restores ADAMTS-13 (A Disintegrin And Metalloprotease with ThromboSpondin type 1 motif) • Requires additional volume
Day 2-7 • Neuro: • Patient remained sedated and paralyzed and her pupils were noted to be reactive sluggishly until 5/13/10 when they were noted to be 8mm and nonreactive • Brain CT was done at that point to assess for new bleed • Diffuse cerebral edema. • Acute extraaxial hemorrhage in the high right parietal region as well as likely thin acute extraaxial hemorrhage along the posteroinferior hemispheric fissure. • 3 mm right to left midline shift. • Effacement of the basilar cisterns with mild medial deviation of the uncus bilaterally which may represent impending uncalherniation.
PICU Day 2-7 • Heme • Patient continued to be severely coagulopathic but labs would improve briefly after each session of plasmapharesis. • Oozing blood from every orifice • Eventually placed on an FFP drip of 20 ml/h and Vit K 5mg IV daily (Day 2) • Clotted off her CVVHD filter twice, so Heparin introduced into circuit and FFP held. • Day 3 PTT was >200, so FFP drip had to be restarted • Daily PRBC and PLT transfusions.
PICU Day 2-7 • ID: • Day 2: ET Cx – C. Albicans, fluconazole added to antibiotic regime • HepBsAg and HepBsAb initially positive (eventually HepBsAg found to be negative) • Malaria and Leptospiral Abs negative • All blood cultures, urine cultures, fluid cultures negative • EBV, CMV, Herpes 1 and 2 IgG all positive – thought to be due to her many transfusions (IgMs all negative) • Dengue PCR negative on Day 5
DENGUE DIAGNOSIS • The diagnosis is mainly clinical but there are laboratory examinations as well • Clinical manifestations range from asymptomatic infection, self-limited dengue fever to DHF with shock syndrome • Symptoms typically develop 4-7 days after being bitten, so often mosquito bites are forgotten • Classic dengue: • Fever accompanied by headache, retro-orbital pain, and marked muscle and joint pain (BONE-BREAK FEVER) • Febrile period may be accompanied by marked fatigue • Rash • GI symptoms : nausea, vomiting and diarrhea • Cough, sore throat, nasal congestion
Dengue Diagnosis • Dengue hemorrhagic fever (DHF) is the most serious manifestation of dengue virus infection and can be associated with circulatory failure and shock. The four cardinal features of DHF, as defined by WHO, include: • Increased vascular permeability (plasma leakage syndrome) evidenced by hemoconcentration (20 percent or greater rise in hematocrit above baseline value), pleural effusion, or ascites • Marked thrombocytopenia (less than 100,000 cells/mm3) • Fever lasting 2 to 7 days. • A hemorrhagic tendency (as demonstrated by a positive tourniquet test) or spontaneous bleeding. • The term dengue shock syndrome (DSS) is used when shock is present
Laboratory testing • Typical Lab findings include: • Leukopenia, thrombocytopenia, elevated AST • Isolation of dengue virus or detection of dengue viral RNA or protein in an acute phase serum or tissue specimen provides the most definitive confirmation of infection. However, the importance of specimen timing and quality and the technical demands of these assays limit their clinical applications. • When laboratory confirmation of illness is obtained it is typically with serology. • Virus isolation and RT-PCR should generally be performed only when needed for epidemiologic purposes or as part of clinical research studies. In the US, most diagnostic laboratory testing for dengue virus infection is performed by the Dengue Branch of the CDC • Serum or plasma are the preferred specimens for virus isolation • Dengue viral proteins can be detected in tissue samples using immunohistochemical staining . Liver tissues appear to have the highest yield. • The dengue viral nonstructural protein 1 (NS1) can be detected in plasma, especially during the first five to six days of illness.
Laboratory Detection • Serology: • The most frequently used serologic tests for the diagnosis of acute dengue virus infection are the hemagglutination inhibition (HI) assay and IgG or IgM enzyme immunoassays. Complement fixation and neutralizing antibody assays are more technically demanding and are used in specialized laboratories only. • The HI assay historically has been and remains the gold standard for serologic testing for dengue virus-specific antibodies. Analysis of paired acute and convalescent serum samples is essential; a fourfold or greater rise in HI antibody titer between acute and convalescent samples defines acute infection. However, cross-reactivity with other flaviviruses has been reported • The antibody response will depend on whether the patient has primary or secondary dengue virus infection. In primary infection, HI antibodies develop late (after the fifth day of illness) and reach titers of less than 1:1250 in the convalescent phase. By contrast, HI antibodies rise early in secondary infection and reach titers above 1:1250 (often 1:10,240 or higher) in the convalescent phase.
Differential Diagnosis of Dengue • Dengue virus infection should be considered in the differential diagnosis of a febrile illness in any patient who has resided in or traveled to an appropriate region in the two weeks before the onset of illness. In patients with the features of DF, the differential diagnosis includes: influenza, enteroviral infection, measles, and rubella • Puerto Rico, the U.S. Virgin Islands, Samoa and Guam are endemic for the virus
PICU Day 8-10 • Dengue titres: • IgG 8.38 • IgM 4.17 • Repeat ET culture once again showed C. Albicans along with aspergillus species so Fluconazole was continued • Continued to require frequent transfusions and FFP drip • Still anuric, CVVHD continuing • New CT done on Day 8 as pupils once again fixed at 7mm - small new bleed anteriorly along corpus callosum but no new mass effect or herniation
PICU Day 8-10 • Still intubated on HFOV and oxygenating slightly better but increased CO2 retention. Decision made to switch to conventional vent so that paralysis could be weaned and a better handle on her neurological status obtained • She continued to have fixed, dilated pupils despite CT suggesting no herniation or worsening edema • Day 8 –PDS attempted to close abdomen, found gallbladder to be necrotic and liver extremely fibrotic. • No cholecystostomy tube placed as she was deemed too ill at that time • Serum ammonia continued to rise and chances of transplant were put rest for the moment as patient was simply too sick to even consider it • DNR order in place
PICU Day 8-10 • Ceftriaxone replaced with Meropenem due to finding of gallbladder necrosis • On Day 9, KK looked to be improving, her sats were up, pCO2 down and her pupils were once again reactive • PDS placed cholecystostomy tube and liver biopsy done • Versed discontinued • Twitch test done 24 hours after Versed and Roc discontinued yielded negative results • Very difficult to visualize fundus even with ophthalmology consult due to severe corneal abrasion, and disc margins noted to be unclear