Download

1 / 23
230 likes | 253 Views
Delve into the complexity of immune checkpoint inhibitors in multiple myeloma, deciphering resistance mechanisms through a variety of factors and potential therapeutic targets.

E N D
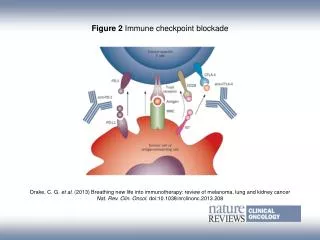
Mechanisms of resistance to Immune checkpoint blockade Barbara Castella, PhD Laboratory of Blood Tumor Immunology (LBTI)Dept of Molecular Biotecnologies and Health Sciences University of Turin
Cancer immunotherapy as the Breakthrough of the last years Immune checkpoint inhibitors
ICP blockade in multiple myeloma: though very promising pre-clinical evidences …… The PD-1/PD-L1 axis modulates the natural killer cell versus multiple myeloma effect: a therapeutic target for CT-011, a novel monoclonal anti-PD-1 antibody. Benson DM Jr, Bakan CE, Mishra A, Hofmeister CC, Efebera Y, Becknell B, et al. Blood. 2010;116(13):2286-94 Immunosuppressive effects of multiple myeloma are overcome by PD-L1 blockade. Hallett WH, Jing W, Drobyski WR, Johnson BD. Biol Blood Marrow Transplant 2011; 17(8):1133-45 PD-L1/PD-1 presence in the tumor microenvironment and activity of PD-1 blockade in multiple myeloma. Paiva B, Azpilikueta A, Puig N, Ocio EM, Sharma R, Oyajobi BO, et al. Leukemia 2015; 29(10):2110-3 Targeting PD1–PDL1 immune checkpoint in plasmacytoid dendritic cell interactions with T cells, natural killer cells and multiple myeloma cells. A Ray, DS Das, Y Song, P Richardson, NC Munshi, D Chauhan, et al. Leukemia. 2015; 29(6): 1441–1444.
…… clinical results have failed to confirm the excellent premises of experimental data Preliminary results of a phase I study of Nivolumab (BMS-936558) in patients with relapsed or refractory lymphoid malignancies. Lesokhin AM, Ansell SM, Armand P, Scott EC, Halwani A, Gutierrez M et al. Blood 2014; 124: 291. The failure of immune checkpoint blockade in multiple myeloma with PD-1 inhibitors in a phase 1 study. Suen H, Brown R, Yang S, Ho PJ, Gibson J, Joshua D. Leukemia. 2015 Jul;29(7):1621-2. Nivolumab in patients with relapsed or refractory hematological malignancy: preliminary results of a phase Ib study. Lesokhin AM, Ansell SM, Armand P, et al. J Clin Oncol 2016; 34:2698-704 Targeting the PD-1/PD-L1 axis in multiple myeloma: a dream or a reality? Rosenblatt J, Avigan D. Blood 2017; 129(3):275-279
Resistance mechanisms to ICP therapy ICP blockade Primary Resistance Sensitive Acquired Resistance Adapted from Wang W., International Immunopharmacology 2017
Major factors contributing to primary resistance to ICP therapy Pitt JM et al., Immunity 2016
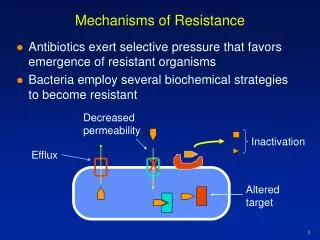
Mechanisms of primary and adaptive resistance to ICP therapy Tumor-Intrinsic factors Absence of antigenic proteins (low mutational burden) Absence of antigen presentation (deletion in TAP, deletion in B2M, silenced HLA) Alteration of several signaling pathways (MAPK, PI3K, WNT, IFN) Sharma P. et al. Cell 2017
Mechanisms of primary and adaptive resistance to ICP therapy Tumor-Extrinsicfactors Absence of T cells (lack of T cells with tumor-Ag specific TCR) Inhibitory immune checkpoints (PD-1, VISTA, LAG-3, TIM-3) Immune suppressivecells (TAMs, Tregs, MDSC) Sharma P. et al. Cell 2017
There is an urgent need of in vitro and in vivo models to identify mechanisms of resistance to ICP blockade and biomarkers of clinical outcome
Vγ9Vδ2 T cells in the bone marrow of myeloma patients: a paradigm of microenvironment-induced immune suppression Very attractive candidates for adoptive immunotherapy in myeloma Vγ9Vδ2 T cells Natural inclination to react against malignant B cells Castella B. et al, Cell Mol Life Sci. 2011; 68(14):2419-32
Intra-tumoral Vγ9Vδ2 T cells are the most significant favorable cancer-wide prognostic population Genltes AJ, Nat Med. 2015 Aug;21(8):938-45
Phosphoantigen reactivity: surrogate assay to interrogate V9V2 T-cell immunocompetence Synthetic phosphoantigen (BrHPP/ CHDMAPP)
Why Vγ9Vδ2 T cells as investigational tools to address the mechanisms of resistance to ICP blockade? IL2 IL2 V9V2 T cells show a tumor-induced hypo-responsiveness to pAg stimulation ZA+IL2 ZA+IL2 BM αβ reactivity BM γδ reactivity 100 80000 CD4 Pooled data Head-to-head CD8 80 40000 ° 60000 * 60 % Proliferating cells (CFSE) 40 30000 40000 20 °p<0,001 *p=0,014 Viable Vγ9Vδ2 T cells/well 0 medium OKT3+αCD28 20000 20000 Viable Vγ9Vδ2 T cells/well * 0 10000 ° 0 PBMC (n=50) BMMC (n=70) PBMC (n=13) BMMC (n=13) CSFE Castella B et al. Oncoimmunology. 2015 May 26;4(11):e1047580
Why Vγ9Vδ2 T cells as investigational tools to address the mechanisms of resistance to ICP blockade? ^ ° § * V9V2 T cells are PD-1+ in the BM of MM patients 30 IL2 25 60 ZA+IL2 ^ ° * * ° ^ 20 20 45 % Vγ9Vδ2+ PD1+ T cells day7 15 ^ * % out ofVγ9Vδ2 + T cells % Vγ9Vδ2+ PD-1+ T cells ° 10 30 § ^ 10 * ° ^ * 15 ° 5 0 CTRL (n=3) MM (n=8) CTRL (n=7) MM (n=13) 0 0 BM (n=8) PB (n=35) BM (n=68) PB (n=18) Naive PD1+ CM PD1+ EM PD1+ TEMRA PD1+ PB BM CTRL MM Castella B, et al. Oncoimmunology. 2015 May 26;4(11):e1047580
Why Vγ9Vδ2 T cells as investigational tools to address the mechanisms of resistance to ICP blockade? 80 100 60 Increased PD-L1 expression in MM BM microenvironment 80 60 PD-L1+ PD-1+ 40 60 40 % CD138+ positive cells % CD44+CD105+ positive cells ° ^ % MDSC positive cells 40 20 20 20 ^ 0 0 0 PD-1 PDL1 BM MM (n=26) PB (n=12) BM (n=9) PB (n=12) BM (n=50) ° BMSC MM CTRL MM Castella B, et al. Oncoimmunology. 2015 May 26;4(11):e1047580
Why Vγ9Vδ2 T cells as investigational tools to address the mechanisms of resistance to ICP blockade? PD-1 blockade only partially recovers BM Vγ9Vδ2 T-cell reactivity in MM patients p < 0.05 70 60000 60 50 40000 40 % Vγ9Vδ2+ CD107+ Viable Vγ9Vδ2 T cells/well 30 20000 20 10 0 0 IL-2 ZA α-PD-1 + - - + + - + - + + + + + - - + + - + + + (0.1) + + + (1) + + + (30) IL-2 ZA α-PD-1 (μg/ml) Castella B, et al. Oncoimmunology. 2015 May 26;4(11):e1047580
Which are the mechanisms responsible for resistance to PD-1 blockade in tumor-experienced Vγ9Vδ2 T cells?
Adaptive resistance to PD-1 blockade in solid tumors The addition of TIM-3 blocking antibody induces a survival advantage Adaptive resistance to anti-PD1 blockade is associated with TIM-3 up-regulation
Immune checkpoint signalling pathways to identify shared molecular targets to overcome resistance to ICP blockade Jing L. et al. Current Opinion in Immunology 2017
Conclusions and challenges Combination with conventionaltherapy (Radiotherapy, Chemotherapy, Targetedtherapy) Modulating immune suppressive tumormicroenvironment and breaking the inhibitory status Strategies to overcome ICP resistance Detection and understanding of the patients’ genetic and epigenetic information of tumor and immunocytes Understanding and exploringupstreamregulators and downstream signaling and target of ICP
Conclusions and challenges Metabolic modulators IDO inhibitors anti-CD73 A2AR inhibitors Immune stimulatory agent anti-41BB/CD137 anti-OX40 anti-ICOS Multiple ICP blockade anti-TIM-3 anti-LAG3 Anti-TIGIT Cancer vaccines DC vaccine peptide vaccine Combination therapies to overcome ICP resistance Epigenetic modifications Histone deacetylase inhibitors hypometilating agents Radiation therapy Immune modulators TGFb inhibitors glutaminase inhibitors CXCR4 inhibitors Targeted therapies VEGF inhibitors BRAF+MEK inhibitors PI3K inhibitors
Credits Laboratory of Blood Tumor Immunology, CeRMS, Torino Prof. Massimo Massaia Myriam Foglietta Ezio Tripoli Claudia Giannotta Chiara Riganti Division of Hematology, AO S. Croce e Carle, Cuneo Mariella Grasso Margherita Bonferroni Claudia Castellino Daniele Mattei Nicola Mordini Davide Rapezzi Roberto Sorasio Division of Hematology, A.O.U. Citta della Salute e della Scienza di Torino (Prof. Mario Boccadoro) Alessandra Larocca Stefania Oliva Paola Omedè Vittorio Muccio Laboratory of Angiogenesis and Immunology, Bari Prof. Angelo Vacca Roberto Ria Assunta Melaccio Laboratory of Immunogenetics, Turin Prof. Fabio Malavasi Angelo Corso Faini Yulia Yakymiv