Background (1)
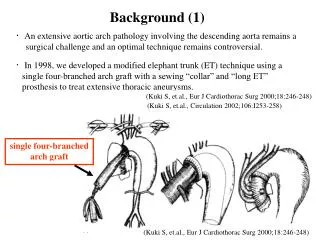
Background (1). ・ An extensive aortic arch pathology involving the descending aorta remains a surgical challenge and an optimal technique remains controversial.

Background (1)
E N D
Presentation Transcript
Background (1) ・An extensive aortic arch pathology involving the descending aorta remains a surgical challenge and an optimal technique remains controversial. ・In 1998, we developed a modified elephant trunk (ET) technique using a single four-branched arch graft with a sewing “collar” and “long ET” prosthesis to treat extensive thoracic aneurysms. (Kuki S, et.al., Eur J Cardiothorac Surg 2000;18:246-248) (Kuki S, et.al., Circulation 2002;106:I253-258) single four-branched arch graft (Kuki S, et.al., Eur J Cardiothorac Surg 2000;18:246-248)
Background (2) ・We have made minor changes to the original technique and applied this technique for a wide variety of aortic pathologies. (Hara H, et.al., J Thorac Cardiovasc Surg 2009;137:777-778) (Taniguchi K, et.al., Ann Thorac Surg 2007;84:1729-34) (Shudo Y, et.al., Ann Thorac Surg 2007;84:659-661) Objectives In this study, we investigate the early operative results and long-term outcome of total arch replacement with long ET in 132 consecutive patients since October 1998.
Operative strategies Onthebasisofthe “uninvolved” descendingaortadiameter(atTh6-Th8),oneofthetwofollowingstrategieswasadoptedin principle. ・Single-ETstrategy: n=99 ・Descendingaorta:35mm or less. ・The first stage procedure was attempted as a “permanent ET”. 30mm ・Staged-ETstrategy: n=33 ・Descendingaorta:greaterthan35mm. ・Two-stage operation was planned, with the second performed within an appropriate period after the initial operation. 40mm
Operative technique (1) CPB is established via the bicaval and right axillary artery cannulae, and the ascending aorta is incised. While cooling the patient, a proximal anastomosis is performed.
Operative technique (2) Then the patient cooled to 25°C, a long elephant trunk is inserted into the descending aorta aided by a catching catheter under an open distal condition. ET diameter and length: • ET diameter: Undersized by 10-20% of outer diameter of descending aorta at Th6-Th8. • ET length: Determined preoperatively by measuring the aorta from the base of the innominate artery to Th6-Th8. 3-0 Tevdek suture
Operative technique (3) A distal anastomosis is then performed at the base of the innominate artery between the proximal graft and distal aorta, incorporating the ET tube graft. The arch vessels are individually reconstructed while re-warming the patient.
Concomitant Procedures and Operative Data Concomitant Procedures (49 procedures in 46 (35%) patients) Operative Data : Hypothermic circulatory arrest time of the lower body for open distal anastomosis. *
Results (1):Early Mortality and Morbidity Operative mortality (≤30 days): 2 ( 1.5%) TAAA rupture:2 Hospital mortality (>30 days): 7 ( 5.3%) TAAA rupture: 1, Pneumonia: 2, Mediastinitis: 2 MOF from biliary sepsis: 1, Aorto-esophageal fistula: 1 Hemorrhagic complication Re-exploration for bleeding: None Neurological complications Permanent stroke: 3 (2.3%) Paraplegia: 3 (2.3%), Paraparesis: 1 (0.8%) Transient paraplegia (recovered within 24 hours): 4 (3.0%) Recurrent nerve palsy (new-onset), Phrenic nerve palsy: None Downstream operation (rapid 2-stage surgery) Thoracotomy approach: 12 Transluminal approach (TEVAR): 8
Results (2): Complete thromboexclusion around ET Single-ETstrategy Staged-ETstrategy (n=99) (n=33) Success Success Failure Failure n=13 n=11 n=22 (67%) n=86 (87%) Failure of thromboexclusion N=22 (67%) Second-stageprocedure: 16 Being followed: 2 Aortic rupture: 4* Failure of thromboexclusion N=13 (13%) Second-stageprocedure: 11 Being followed: 2 Aortic rupture: None (includingthe1patientwhorefusedthesecond-stageoperation) *
Results (3):Late Mortality and Morbidity Aneurysm-related mortality: 4 ( 3%) TAAA rupture: 1, Iliac aneurysm rupture: 1 Aorto-pulmonary fistula: 1, ET graft infection: 1 Aneurysm-nonrelated mortality: 14 ( 10.6%) Pneumonia: 3, Stroke: 3, Neoplasm: 3, Heart failure: 2 Neoplasm: 3, Sepsis: 1, Arrhythmia: 1, Unknown: 1 Subsequent operation : 10 ( 7.6%) Thoracotomy approach: 6, Transluminal approach: 1 Thoracoabdominal aortic repair: 2 Abdominal aortic repair (infra-renal): 1 Late complications Aorto-esophageal fistula (alive): 1 Distal aneurysm expansion: None Peripheral thromboembolism: None
Results (4): Survivals (Average follow up: 45 ± 37 months) 100 89% 86% 80% 77% 80 68% Percent survival (%) 60 40 Patients at risk: 20 102 80 67 52 42 36 25 17 0 Months after operation
Conclusion Most patients assigned to the single-stage strategy showed complete thromboexclusion of the perigraft space around the ET with lowering the need for a second-stage procedure. In addition, most patients assigned to the two-stage strategy showed persistent perigraft perfusion around the ET and required a rapid second-stage procedure. Our procedure with long ET for arch aneurysms using an undersized graft is uniformly applicable for a wide variety of aortic pathologies with achieving satisfactory short-term and long-term outcomes.