Download
1 / 35
380 likes | 464 Views
Explore the process of healing, acute phase response, and sepsis as well as the mechanisms involved in tissue repair, stem cells, and regeneration. Learn about inflammatory stimuli, immune responses, and organ failure in the context of restoring structure and function.

E N D
Healing and tissue repair Assist.Prof.Dr. Baydaa H.Abdullah
Systemic inflammatory response • Acute Phase Response • Fever • Acute-phase protein secretion from liver • Leukocytosis • Tachycardia, increased blood pressure • Shivering, chills • Anorexia, somnolence, malaise • Septic shock
Acute Phase Proteins • Secretion of Acute Phase proteins by the liver • C-reactive Protein (CRP) • Serum Amyloid A (SAA) • Serum Amyloid P (SAP) • Complement • Fibrinogen • Prothrombin • Ferritin • Ceruloplasmin • α1-antitrypsin • α2-macroglobulin • Acute phase proteins bind: • Microbial constituents, acting as opsonins to fix complement • Chromatin, aiding early clearing of necrotic cells
Autonomic and Behavioral Responses • Autonomic • redirection of blood flow from cutaneous to vascular bed • increased pulse and blood pressure • decreased sweating • Behavioral • Rigors (Shivering) • Chills • Anorexia • Somnolence • Malaise
Sepsis • Systemic Inflammatory Response Syndrome involves two or more of the following • temperature >38.3ºC or <36ºC • heart rate >90 beats/min; <32 mm Hg • respiratory rate >20 breaths/min, PaCO2 or need for mechanical ventilation • WBC count >12,000/uL or <4,000/uL or >10% immature forms (bands) • Sepsis is defined as SIRS associated with suspected or confirmed infection--positive blood cultures are not necessary • Severe sepsis is sepsis complicated by a predefined organ dysfunction • Septic shock is cardiovascular collapse (hypotension) related to severe sepsis despite adequate fluid resuscitation
Septic stimuli • Gram-negative bacteria • LPS, endotoxin • Binds to LPS binding protein (LBP) • Binds to CD14 opsonin receptor • TLR-4 binds LPS and LPS-LBP • Stimulates release of TNF, IL-1, IL-6 • Gram-positive bacteria • Exotoxins, superantigens • Bind Vb regions of TCRs and/or to MHC-II • TLR-2 binds cell wall components • Stimulates release of IFN-g, TNF, IL-1, IL-6
Progression of sepsis • Cytokine release and amplification • Vasular response and neutrophil migration • Coagulation cascade • Counter-inflammatory response • Apoptosis of Th and B-cells • Systemic acute phase response • increased cortisol production and release of catecholamines • upregulation of adhesion molecules • release of prostanoids and platelet-activating factor (PAF) • Organ failure
Multiple organ failure • Neutrophils damage tissue directly by releasing lysosomal enzymes and superoxide-derived free radicals • TNF-α induces nitric oxide synthase • nitric oxide causes further vascular instability • contributes to direct myocardial depression • Widespread vasodilation • Decreased production of vasopressin (ADH) and glucocorticoids • Circulatory collapse and tissue hypoxia
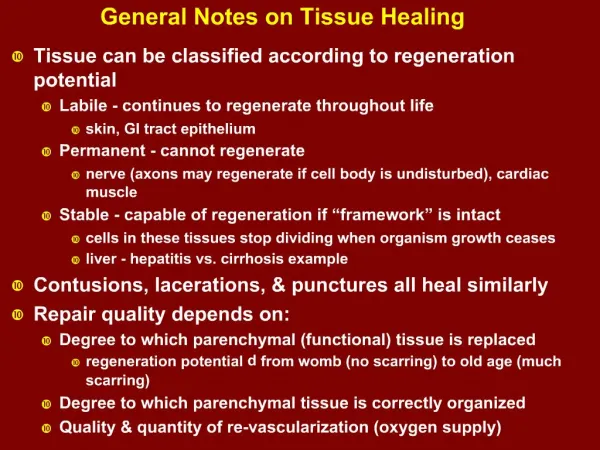
Restoration of Structure and Function • Occurs if connective tissue structure relatively intact • Surviving parenchymal cells must have the capacity to regenerate • Labile Cells • Actively divide throughout life • cells of the epidermis and gastrointestinal mucosa • cells lining surface of the genitourinary tract • hematopoietic cells of the bone marrow • Stable Cells • Undergo few divisions normally, but can be activated from G0 cells when needed • hepatocytes • renal tubular cells • parenchymal cells of glands • mesenchymal cells (smooth muscle, cartilage, connective tissue, endothelium, osteoblasts)
Regeneration • Proliferation of cells and tissues to replace lost structures • Whole organs and complex tissues rarely regenerate after injury • Compensatory growth rather than true regeneration • Liver hypoplasia and kidney hypertrophy • Continuously renewing tissues regenerate after injury if tissue stem cells are not destroyed
Stem Cells • Characterized by self-renewal properties and capacity to generate differentiated cell lineages • embryonic stem cells (ES cells) are pluripotent • adult (somatic) stem cells are restricted by niche • skin, gut lining, cornea, hematopoietic tissue
Stem Cells in Homeostasis and Healing • Bone marrow • Hematopoietic Stem Cells generate all of the blood cell lineages • Marrow Stromal Cells generate precursors of tissue to which migrated • Liver • Oval cells are bipotential progenitors of hepatocytes and biliary cells • Brain • Neural precursor cells generate neurons, astrocytes, and oligodendrocytes • Skin • Hair follicle bulge, interfollicular areas of the surface epidermis, and sebaceous glands • Intestinal epithelium • crypts are monoclonal structures derived from single stem cells • villus contains cells from multiple crypts • Skeletal and cardiac muscle • satellite cells beneath the myocyte basal lamina generate differentiated myocytes after injury • Cornea • limbal stem cells maintain corneal transparency
Proliferative capacity of tissues • Labile tissues • Continuously dividing tissues containing stem cells • Stable tissues • Parenchymal cells of solid organs in G0 • Endothelial cells, fibroblasts, smooth muscle • Limited regeneration after wounding • Permanent tissues • Absolutely nonproliferative • Cardiac muscle, neurons
Growth factors • Polypeptides that promote survival and proliferation by signal transduction • Increase in cell size • true growth factors • Increase in cell number • mitogens • Protection from apoptosis • survival factors
Growth Factor-mediated Proliferation • Platelet Derived Growth Factor (PDGF) • promotes the chemotactic migration of fibroblasts and smooth muscles • chemotactic for monocytes • competence factor that promotes the proliferative response of fibroblasts and smooth muscles upon concurrent stimulation with progression factors • Epidermal Growth Factor (EGF) • promotes growth for fibroblasts, endothelial and epithelial cells • is a progession factor - promotes cell-cycle progression. • Fibroblast Growth Factor (FGF) • promote synthesis of fibronectin and other extracellular matrix proteins • chemotactic for fibroblast and endothelial cells • promotes angiogenesis • links extracellular matrix components (collagen, proteoglycans) and macromulocules (fibrin, heparin) to cell-surface integrins. • Transforming Growth Factors (TGFs) • TGF-α - similar to EGF • TGF-β - mitosis inhibitor that aids in modulating the repair process. May be responsible for hypertrophy by preventing cell division. Chemotactic for macropahges and fibroblasts • Macrophage-derived cytokines (IL-1 and TNF) • promote proliferation of fibroblasts, smooth muscle and endothelial cells
Repair Process • Removal of Debris • begins early and initiated by liquefaction and removal of dead cells and other debris • Formation of Granulation Tissues • connective tissue consisting of capillaries and fibroblasts that fills the tissue defect created by removal of debris • Scarring • fibroblasts produce collagen until granulation tissue becomes less vascular and less cellular • progessive contraction of the wound occurs, resulting in deformity of original structure
Tissue Repair • Necessary when barriers are penetrated • Cells must divide and migrate • Occurs in two major ways • Regeneration • Same kind of tissue replaces destroyed tissue • Original function restored • Fibrosis • Connective tissue replaces destroyed tissue • Original function lost
Slide 1 Figure 4.12. Tissue repair of a nonextensive skin wound: regeneration and fibrosis. Scab Epidermis Vein Blood clot in incised wound Inflammatory chemicals Migrating white blood cell Artery Inflammation sets the stage: • Severed blood vessels bleed. • Inflammatory chemicals are released. • Local blood vessels become more permeable, allowing white blood cells, fluid, clotting proteins, and other plasma proteins to seep into the injured area. • Clotting occurs; surface dries and forms a scab.
Regenerating epithelium Area of granulation tissue ingrowth Fibroblast Macrophage Budding capillary 2 Organization restores the blood supply: • The clot is replaced by granulation tissue, which restores the vascular supply. • Fibroblasts produce collagen fibers that bridge the gap. • Macrophages phagocytize dead and dying cells and other debris. • Surface epithelial cells multiply and migrate over the granulation tissue.
Steps in Tissue Repair • Regeneration and fibrosis • The scab detaches • Fibrous tissue matures; epithelium thickens and begins to resemble adjacent tissue • Results in a fully regenerated epithelium with underlying scar tissue
Slide 3 Figure 4.12. Tissue repair of a nonextensive skin wound: regeneration and fibrosis. Regenerated epithelium Fibrosed area Regeneration and fibrosis effect permanent repair: • The fibrosed area matures and contracts; the epithelium thickens. • A fully regenerated epithelium with an underlying area of scar tissue results. 3
Healing and granulation • Fibroplasia is a response to • Damaged connective tissue • Parenchymal damage exceeds regenerative capacity • Hyperplasia of connective tissue • Neovascularization • Granulation • coordinated proliferation of fibroblasts with a rich bed of capillaries • intensely hyperemic with a roughened or granular, glistening surface • healthy granulation tissue resists secondary infections
Healing by First Intention • Clean, surgical incision or other clean narrow cut • Focal disruption of epithelial basement membrane with little cell damage • Regeneration dominates fibrosis • Scabbing with fibrin-clotted blood • Neutrophils migrate to edges • Epidermis becomes mitotic and deposits ECM • Macrophages replace neutrophils • Vascularization and collagen deposition fills gap • Contraction of collagen minimizes epidermal regeneration
Healing by Second Intention • Larger area of tissue injury such as abcess, ulcer, infarction that destroys ECM • Large clot or scab with fibrin and fibronectin fills gap • Larger volume of necrotic debris must be removed by more neutrophils and macrophages • Opportunity for collateral damage by phagocytes • Scar tissue formed from vascular cells, fibroblasts, and myofibroblasts • Contraction of myofibroblasts distorts tissue • More prone to infection
Regenerative Capacity in Different Tissues • Regenerate extremely well • Epithelial tissues, bone, areolar connective tissue, dense irregular connective tissue, blood-forming tissue • Moderate regenerating capacity • Smooth muscle and dense regular connective tissue • Virtually no functional regenerative capacity • Cardiac muscle and nervous tissue of brain and spinal cord • New research shows cell division does occur • Efforts underway to coax them to regenerate better
Aging Tissues • Normally function well through youth and middle age if adequate diet, circulation, and infrequent wounds and infections • Epithelia thin with increasing age so more easily breached • Tissue repair less efficient • Bone, muscle and nervous tissues begin to atrophy • DNA mutations possible increased cancer risk
Factors that Impede Repair • Retention of debris or foreign body • Impaired circulation • Persistent infection • Metabolic disorders • diabetes • Dietary deficiency • ascorbic acid • protein