Download
1 / 75
781 likes | 1.26k Views
Explore the causes, symptoms, and forms of mechanical jaundice, including obstructive conditions like choledocholithiasis and sclerosing cholangitis. Learn how bile duct diseases and tumors can lead to jaundice and understand the physical signs associated with this condition.

E N D
ETIOLOGY OF THE MECHANICAL JAUNDICE MJ (obturative, obstructive, subhepatic) is the pathologic state, conducting with the jaundice of the skin, skleras, mucous shells as a result of increasing of bilerubin in blood, developing because of different pathologic processes, induct the obturation of the bile ducts
Main reasons of the mechanical jaundice Diseases of ducts External compression Parasite invasion Concrement Innate (cysts, atresias) Choledocholithyasis Tumors (of pancreas, liver, gall bladder, big duodenal teat, metastases) Not tumorous (sclerosing, festering cholangitis, strictures, cholangiopathies) Round worms,suckers, Ribbon worms Mirizzi’s syndrome
Choledocholithyasis Choledocholithyasis – is the localization of the concrements in extra- and intrahepatic bile ducts, appears more frequently as a result of migration of the concrements from the gall bladder at the calculous cholecystitis
Mirizzi’s syndrome 1type– the concrement, wedging to the neck of gall bladder, Hartman’s pocket or bladder’s duct, compresses the common bile duct from the outside 2 type- development of the bedsore with the formation of the cholecystocholedochial fistula
Atresia of the extrahepatic ducts Atresy of the extrahepatic ducts – is characterized with the full defeat of the bile’s evacuation as a result of full obliteration of the extrahepatic ducts
Cysts of the bile ducts Cysts of the bile ducts – is the extension of the intra- and extrahepatic bile ducts
Posttraumatic strictures of the bile ducts Posttraumatic strictures of the bile ducts – it is the strictures of the bile ducts as a result of their defeat Classification of the posttraumatic strictures of the bile ducts By the degree of stricture Full Not full By the level of defeat High Low By the clinic currency With the jaundice With the cholangitis With the external bile fistula With the biliar cirrhosis of liver By the duration of defeat Limited (to 1 sm) Spreaded (1-3 sm) Subtotal (over 3 sm) Total
Primary sclerosing cholangitis Primary sclerosing cholangitis – idiopathic disease, characterised with the diffuse inflammation and fibrosis of the bile ducts 1.PSC, not connected with other additional diseases 2.PSC, developing on the background of inflammatory diseases of intestines (ulcer colitis, Crone’s disease) 3.PSC, connected with the system fibrous changes (retroperitoneal fibrosis, Veber-Crengen’s disease, Ridel’s thyreoditis, mediastinal fibrosis) 4.PSC, connected with other autoimmune diseases (lupus, RA, diabetes 1 type, Shegren’s disease) 5.At some cases the development of the PSC connect with the development of immune deficit, as innate, so obtained (AIDS and other)
Secondary sclerosing cholangitis Secondary sclerosing cholangitis unites the group of cholangitis with the directly stated etiologic factor The reasons of the secondary sclerosing cholangitis 1.Choledocholithyasis 2.Postoperative scare strictures 3.Fungous infection 4.Parasite invasion 5.Pancreatitis 6.Intraductal and intraarterial introducing of some medicines 7.Ischemia as a result of trauma of the vessels 8.Cholangiocarcinoma or limphoma
Recidivate festering cholangitis Recidivate festering cholangitis – develops after passed cholangitis as a result of not adequate sanation of the bile ducts Incitants of the RFC Gram negative, conditionally pathogeneous flora, less – anaerobe infection Clinic picture Pain in the right under-rib, high temperature with the shiverings, slow progressive jaundice
Tumorous defeats of the bile ducts 1. Tumors of the pancreas’s head 2. Tumors of the big duodenal teat 3. Tumors of the liver’s gates 4.Tumors of the gall bladder 5. Secondary (metastatic) defeat of the perycholedochial lymph nodes
External compression of the bile ducts Tumorous defeat of the hepatobiliar zone Tumors of the pancreas’s head, tumors of the big duodenal teat, tumors of the liver’s gates, gall bladder, secondary (metastatic) defeat of the perycholedochial lymph nodes Inflammatory diseases Pancreatitis, cysts of the pancreas, papillitis, diverticulitis, perycholedochial lymphadenitis, postbulbar ulcer of the duodenum, parapapillar or perypapillar divrticulitis Diseases of the vesselsAneurisms of the hepatic artery, abdominal aorta, cavernous transformation of the portal vein
Parasite invasion of the bile ducts Round worms (ascarides, hair-head) Suckers (two-moustaches of cats, hepatic) Ribbon worms (bull cepen, pig cepen, echinococc)
The main clinic symptoms at the mechanical jaundice Jaundice of the skin, scleras; Skin scratching; Discoloration of the excrements; Darkening of urine.
Clinic forms of the mechanical jaundice Jaundice-painful form Jaundice-pancreatic form Jaundice-septic form Jaundice-not painful form Jaundice-cholecystitis form
Physical data at the mechanical jaundice • Jaundice of the skin, scleras, mucous shells; • High temperature; • Light (acholic) excrement; • Urine with a color of beer or strong tea; • Increased sizes of liver and gall bladder; • Pain in the right under-rib; • Formation in the abdominal cavity at the palpation; • Curvuaz’e’s syndrome.
Laboratory data at the mechanical jaundice • Hyperbilerubinemia because of direct fraction; • Increased level of the hepatic fraction of alkaline phosphatas of blood; • High level of bile acids; • Hypercholesterinemia; • Absence of the stercobilin in the excrement, urobilinogen in the urine; • Increased content of the bile pigments in urine.
It is the complex of symptoms, characterized with the defeat of one or many functions of the liver as a result of acute or chronic defeat of its parenchima, at which there is no correspondence between requirements of the organism and possibilities of the liver in satisfaction of these requirements. Hepatic insufficiency
Clinic stages of the hepatic insufficiency Istage of the hepatic insufficiency IIstage of the hepatic insufficiency IIIstage of the hepatic insufficiency
Clinic picture at theIstage of the heepatic insufficiency The state is satisfactory, asthenovegetative, dyspeptic, painful syndromes.Cholestatic syndrome.Jaundice of the scleras, skin, increasing of the liver; hypoalbuminemia. Cytolitic syndrome.Subicterous scleras, the liver is increased, compact concentration, its border is sharp, sometimes the spleen is increased; Субиктеричность склер, печень умеренно увеличена, плотной консистенции, край её заострен, иногда увеличена селезенка;hypoalbuminemia with dysproteinemia.
Biochemical factors of blood at the first stage of hepatic insufficiency Bilirubin Alkaline phosphatase AST ALT Cholestatic syndrome Cytolitic syndrome
Clinic picture at the II stage of hepatic insufficiency the state is middle: asthenovegetative, dyspeptic syndromes, insomnia, sleepiness in a day, apathy, fever.. Cholestatic syndrome.Jaundice of the scleras, skin with the grey tone, scratching, pain in joints and bones, balloned abdomen, hemorrhages, significant increasing of the liver; its surface is smooth, compact, the border is rounded or sharp, hypoalbuminemia. Cytolitic syndrome.Icterous scleras, skin, vessel’s stars on the skin, the liver is significantly increased, compact concentration, not smooth surface, spleenomegaly with the hyperspleenism; ascitis, varicous extended veins of the esophagus, different hemorrhages, nasal, gastral, uterus bleedings; hypoalbuminemia with dysproteinemia.
Biochemical factors of blood at the first stage of hepatic insufficiency Bilirubin Alkaline phosphatase AST ALT Cholestatic syndrome Cytolitic syndrome
Clinic picture at theIIIstage of the heepatic insufficiency The state is hard or very hard, jaundice of the skin, fever, sometimes the “hepatic” smell from the mouth, hemorrhagic diathesis, significant increasing of liver or its reduction.А – deceleration of the thinking, defeat of sleeping, disorientation, depression or euphoria, sometimes appearance of the tremor of hands. Hypoalbuminemia with dysproteinemia. B– defeat of the consciousness, enxiety with the delirium, sleepiness, disorientation, significant tremor of hands (pre-coma). C – absence of the consciousness, rigid muscles of the head, pathologic reflexes (coma).
Biochemical factors of blood at the third stage of hepatic insufficiency Bilirubin AST ALT
Stages of the diagnostic • careful gathering of the anamnesis, physician examination, using of the screening laboratory researches. • wording of the preliminary diagnosis (suspicion to the obstructive genesis of the jaundice). • choose and indication of the sequence of using of the special instrumental methods of the research for topic diagnostic.
Anamnesis • Presence of the GSD in the anamnesis • Attacks of the pain • Fever, shivering • Operations on the bile ducts in the anamnesis • Firm skin scratching • Loss of the weight • Elder age
Methods of the instrumental diagnostic 1.Not invasive methods: • US • computer tomography 2.Invasive methods : • ERPChG • TTHG
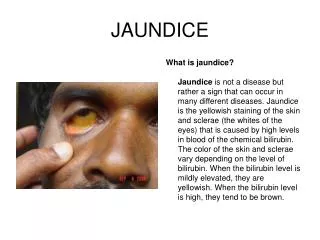
Types of jaundice Hemolytic Parenchimatous Mechanical
Hemolytic jaundice Hemolytic jaundice is conditioned by the increased defeat of the erytocytes or their not developed predecessors. As a result of this the increased formation of the bilerubin begins, that the liver cannot evacuate it fully.
Parenchimatous jaundice Parenchimatous jaundice is conditioned by the defeat of the hepatocytes and bile capillaries, with the increasing of the not direct bilerubin in blood.
Mechanical jaundice Mechanical jaundice develops at the obstacle to the passage of bile from the bile ducts to the duodenum
Differential diagnostic of the jaundices by the clinic signs
When the mechanical character of jaundice is defined it is necessary to carry out the differential diagnostic between the benignus and malignus jaundice to the right choose of the treatment tactic
Differential diagnostic of the mechanical jaundices by the clinic signs
Need of two-stage treatment On the background of the hepatic and renal insufficiency, long lasting at the state of jaundice inducts such changes in the organs and systems that the reconstruction of the normal passage of bile by the one-stage operative way may cause the progressing of the hepatic insufficiency
I stage Drainage Dosed decompression Liquidation of the polyorgan insufficiency
II stage Reconstruction of the normal passage of the bile into the intestine Endoscopic retrograd interventions Transcutaneus transhepatic endobiliar interventions Absence of the effect Open operations
Indications to the endoscopic retrograd interventions extension of the choledoch by the US data over 8 mm discovery of the reasons of the MJ and localization of the pathologic process in the bile ducts hyperbilerubinemia with the bad visualization of the extrahepatic bile ducts by the US data
Contraindications to the endoscopic retrograd endobiliar interventions • Acute infarct • acute breaches of the blood circulation • hard not corrective manifestations of the heart-vassels and breathing insufficiency
Types of the endoscopic retrograd endobiliar interventions Endoscopic retrograd pancreatocholangiography Nasobiliar drainage
Indications to the endoscopic papillosphincterotomy choledocholithyasis stenosing papillitis stenosis of the terminal department of the choledoch and big duodenal teat with the duration to 1,5 sm mechanical jaundice with the hepatic insufficiency of I and II degree
Types of the papillosphincterotomy Papillotomy Subtotal or total papillosphincterotomy Boarded papillosphincterotomy