Jaundice
Jaundice . Presented by Dr. Pollock Prepared by Christopher Edwards Tintanalli Chapter 84, pgs. 560-561 October 2005. Jaundice. Clinical marker of defect in metabolism &/or excretion of bilirubin.


Jaundice
E N D
Presentation Transcript
Jaundice Presented by Dr. Pollock Prepared by Christopher Edwards Tintanalli Chapter 84, pgs. 560-561 October 2005
Jaundice • Clinical marker of defect in metabolism &/or excretion of bilirubin. • ER task to initiate lab eval or imaging studies to identify cause and determine admission or outpt therapy.
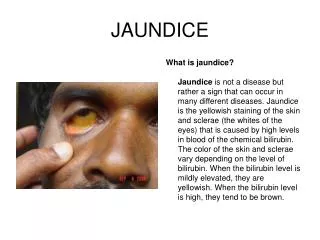
Pathophysiology • Yellow discoloration of sclera, skin, mucous membranes due to deposition of bile pigment • Clinically detected with serum bilirubin 2-2.5mcg/dL or (2 times nl)
What is bilirubin? • The breakdown product of Hgb from injured RBCs and other heme containing proteins. • Produced by reticuloendothelial system • Released to plasma bound to albumin • Hepatocytes conjugate it and extrete through bile channels into small intest.
What causes bilirubin? • Overproduction by reticuloendothelial system • Failure of hepatocyte uptake • Failure to conjugate or excrete • Obstruction of biliary excretion into intestine
Unconjugated production exceeds ability of liver to conjugate Ex. Hemolytic anemias, hemoglobinopathies, in-born errors of metab., transfusion rxn. Conjugated Can produce but not excrete Metabolic defect Intra- or extrahepatic obstruction Unconjugated vs. Conjugated
Clinical Features • Careful history and PE • Family history (Gilbert, Rotor, Crigler-Najjar, Dubin-Johnson, Sickle Cell) • Healthy young person with fever, malaise, myalgias = viral hepatitis (try to locate source)
Clinical Features • Gradually develops symptoms = hepatic/bile duct obstruction (consider ETOH liver dz/cirrhosis) • Develops acutely with abd pain = acute cholangitis 2° to choledocholithiasis
Clinical Features • Painless jaundice in older person with epigastric mass & weight loss = biliary obstruction from malignancy • Hepatomegaly with pedal edema, JVD, and gallop = CHF
Serum bilirubin level (total and direct) Liver aminotransferase levels Alk. Phos U/A for bilirubin and urobilogen CBC PT Other labs pertinent to history Coombs test Hgb electrophoresis Viral hepatitis panel U/S Gallbladder Laboratory Tests
Disposition • Hemodynamically stable, new-onset jaundice, no evidence of liver failure or acute biliary obstruction discharge with follow up • If one of above violated admission with surgery consult
Cholecystitis and Biliary Colic Tintanalli Chapter 85 Pages 561-566
Biliary Tract Emergencies Related to Gallstones • 1) Biliary Colic • 2) Cholecystitis • 3) Gallstone pancreatitis • 4) Ascending cholangitis
Gallstones • Most gallstones are asymptomatic • Usually seen in obese females 20-40 yoa and pregnancy (Remember fat, fertile, flatulent, female, forty) • Associated with upper abdominal pain
Gallstones • Uncommon in children (seen with hemolytic d/o, idiopathic, cystic fibrosis, obesity, ileal resection, long term use of TPN) • Elderly • 14-27% symptomatic gallstone dz. • More likely biliary sepsis/gangrenous GB • perioperative morbidity • Mortality rate 19%
Gallstone Risk Factors • Familial • Asian descent • Chronic biliary tract infections • Parasitic infections (ascaris lumbricoides) • Chronic liver dz (ETOH) • Chronic intravasular dz (Sickle Cell, Hereditary Scherocytosis) • Hepatitis A, B, C, E • HIV • Herpesvirus
Pathophysiology • Bile • Manufactured & secreted from hepatocytes GB storage in canaliculi, ductiles, & bile ducts bile ducts enlarge form R and L hepatic ducts form common hepatic duct joins cystic duct from GB to form CBD Ampulla of Vater duodenum
Pathophysiology • Release of bile stimulated by cholecystokinin secreted from small int. mucosal cells when fats & AA enter duodenum
Pathophysiology • Symptomatic cholelithiasis = stone migration from GB into biliary tract with eventual obstruction obstruction of hollow viscus pain, nausea & vomiting acute cholecystitis
Pathogens Involved in AcuteCholecystitis • E. coli/Klebsiella-70% • Enterococci-15% • Bacteroides-10% • Clostridium-10% • Group D Strep • Staphylococcal species
Clinical Features • Overlap of s/s of PUD, gastritis, GERD, nonspecific dyspepsia • RUQ pain • Upper abd/epigastric pain • Radiation to L upper back • Pain persisant lasting 2-6h
Clinical Features • Clinical studies show no coorelation with fatty food • Peak symptoms 9PM-4AM –follows circadium rhythm • Infrequent pain-intervals more than 1wk • Not related to meals in 1/3 of pts.
Clinical Features of Acute Cholecystitis • Pain lasts beyond 6h • N,V • Anorexia • Fever, chills • +Murphy’s sign ( pain or inspiratory arrest with deep, subcostal palpation on inspiration) • See Table 85-2
5-10% incidence Elderly DM Multiple trauma Extensive burns Prolonged Labor Major surgery GB torsion Systemic vasculitis states Bacterial or parasitic infection of biliary tract Acalculous Cholecystitis
Gastritis GERD Pancreatis Hepatitis PUD AMI in elderly Acute renal colic Acute pyelo Appendicitis (pregnancy, retrocecal) PID Fitzhugh-Curtis Syn. Ectopic Pneumonia Pleural Effusion Differential Diagnosis
Diagnostic Studies • Most important is high clinical suspicion and U/S. • Usually labs nl. (CBC, bilirubin, Alk. Phos, LFTs, U/A, UHCG, Lipase) • CXR- r/o pneumonia, pleural effusion • 12 Lead EKG- r/o ACS • U/S shows stones small as 2mm • CT when ? other intraabdominal path • HIDA Scan
Complications • Fluid & Electrolyte deficiencies- due to vomiting & anorexia • Upper GI hemorrhage- Mallory-Weiss tears • Gallstone pancreatitis • Ascending cholangitis • Cholecystitis • GB Empyema • Emphysematous (gangrenous) GB
Treatment • Uncomplicated Symptomatic Cholelithiasis– No immediate surgery, Elective cholecystectomy, Control symptoms • Antispasmodics • Opiates (Meperidine preferred) • Antiemetics • Ketorolac (relieves GB distention) • Replace fluids & electrolytes
Treatment • Acute Acalculous/Calculous Cholecystitis • If septic – wide spectrum abx and immediate surgery • If not septic – single agent abx (3rd gen cephalosporin), surgery within 24-72 hours
Hepatic Disorders & Hepatic Failure Tintanalli Chapter 86 Pages 566-573
Acute & Chronic Liver Disease • CLD- 12th leading cause of death in US • However, decreased inf with hepatitis viruses A, B, & C in last decade. • Other causes: ETOH, CMV, HSV, Coxsackie, EBV, Drugs, autoimmune, metabolic
Pathophysiology • Hepatocellular • Cholestatic • Immunologic • Infiltrative Disorder
Clinical Features • Acute Viral –anorexia, N, V, low-grade fever • Cholestatic –jaundice, pruritis, clay-colored stools, dark urine • Chronic –complications of advanced cirrhosis, portal HTN (abd pain, ascites, GI bleed, fever, AMS)
History, History, History • Sexual behaviors • Travel • ETOH • Illicit drug use • Natural supplements (Vitamin A) • Herbal remedies • Mushroom ingestion • Raw oysters • Family history
Physical Findings • Acute • Moderate liver enlargement, tenderness, +/- jaundice • Chronic • Sallow complexion, extremity muscle atrophy, palmar erythema, cutan spider nevi, parotid enlargement, testicular atrophy, gynecomastia, splenomegaly, ascites
LFTs • 1) Markers of acute hepatocyte injury & death: AST (SGPT), ALT (SGOT), Alk Phos. • 2) Measures of hepatocyte synthetic fxn : PT, Albumin • 3) Indicators of hepatocyte catabolic activity: direct & indirect bilirubin, ammonia • 4) Others: Lactate dehydrogenase, viral hepatitis serology
Cirrhosis & Complications of End Stage Liver Dz • Gastroesophageal Varices & Hemorrhage • Medical literature shows no evidence of risk of iatrogenic hemorrhage from placement of naso- or orogastric catheters!!! • Tx: Hemodynamic & airway stabiliz. • Endoscopy-banding/sclerotherapy • Vasoactive drugs: Somatostatin, Octreotide • Abx. to cover enteric organisms
Ascites & Spontaneous Bacterial Peritonitis • Paracentesis (U/S guided or not) • Lab Testing of Ascitic Fluid (WBC, diff, glucose, protein, gram stain, C&S) • SBP = WBC>1000/L, low glucose, high protein • Abx coverage of enterobacteriaceae (63%), S. Pneumoniae (15%), Enterococci (6-10%), Anaerobes (<1%) • See table 86-4
Hepatorenal Syndrome • Acute renal failure with acute or chronic hepatic failure • Etiology unknown • Median survival 21 days • Tx: Liver transplant & kidneys will spontaneously recover
Hepatic Encephalopathy • Accumulation of nitrogenous waste products • Diagnosis of exclusion • Tx: Decreased protein intake, lactulose (traps ammonia & allows stool excretion), neomycin
THE END!!! • Questions???????
Questions • 1) Unconjugated hyperbilirubinemia usually results from a intra- or extrahepatic biliary obstruction. • A. True • B. False • 2) All patients with jaundice should be admitted to the hospital for further workup. • A. True • B. False
3) All of the following are risk factors for development of gallstones except: • A. Pregnancy • B. >50 yoa • C. Female • D. Obesity • E. Asian descent
4) Clinical features of cholecystitis include all of the following except: • A. RUQ abdominal pain • B. Radiation to R upper back • C. Nausea, Vomiting • D. + Murphy’s sign • E. Fever
5) A marker of acute hepatocyte injury &/or hepatocyte death is: • A. PT • B. ALT • C. Albumin • D. Direct bilirubin • E. Ammonia
Answers • All answers are B!!