Download
1 / 32
320 likes | 336 Views
Learn about gestational diabetes mellitus (GDM) and preexisting diabetes screening, diagnosis, and management in pregnancy. Understand the etiology, pathophysiology, and risk factors for GDM. Discover why early detection and treatment are crucial for both mother and baby's health.

E N D
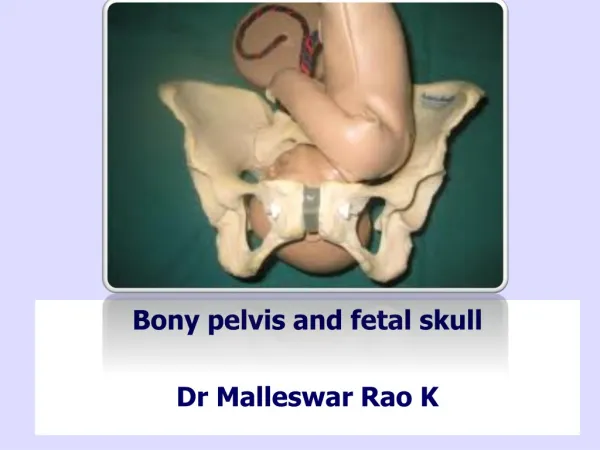
GESTATIONALDIABETES MELLITUS & Preexisting (Overt) Diabetes(Screening, Diagnosis, Management and Follow-up) Dr Malleswar Rao Kasina, MD,DGO
White classification • Based on maternal and obstetric risk factors, graded from A (best) to F (worst) designed to predict pregnancy outcomes
1971 and further updated in 1980 to incorporate ischemic heart disease and renal transplantation
Introduction Gestational diabetes mellitus (GDM): Diabetes diagnosed in the second or third trimester of pregnancy that is not clearly overt diabetes. (American Diabetes Association, 2017)
DEFINITION & MAGNITUDE • A carbohydrate intolerance of varying degrees & severity with onset or first recognition during pregnancy with a probable resolution after the end of pregnancy • Not the same as Type 1 or Type 2 Diabetes • Varies worldwide & among different racial and ethnic groups within a country • Prevalence in India: • Chennai : 0.56% (Ramachandran A, 2002) • Mysore Parthenon Study: 6% ( Fall C,2000)
DEFINITION OF GDM • GDM is defined as any degree of glucose intolerance with onset or first recognition during pregnancy. • and disappear after 6 weeks post partum • After 6 weeks post partum , if MGTT • NORMAL = GDM • ABNORMAL = TYPE 2 DM Source: American Diabetes Association 2009
ETIOLOGY • Pregnancy pro-diabetic state • Pregnancy marked insulin resistance increased insulin requirement GDM • Complicates 4% of all pregnancies • 60% to 80 % of women with GDM are obese & experience insulin resistance & GDM
MECHANISM OF INSULIN RESISTANCE • The pancreas releases 1.5–2.5 times more insulin in order to respond to the resultant increase in insulin resistance.Normal patient meets the demand • In GDM : • Post receptor defect. Inadequate insulin release
Pregnancy Pathophysiology • Glucose is a teratogen at high levels • Crosses placenta readily while insulin cannot • Insulin resistance occurs because hormonal changes associated with pregnancy partially block the effects of insulin • Insulin resistance causes glucose to be shunted from mother to the fetus to facilitate fetal growth and development
Subsequent increase in insulin resistance causes maternal glucose levels to increase 80% of non-pregnant women Increased insulin resistance Decreased insulin secretion Increased maternal glucose GDM • GDM disappears after pregnancy • Useful physiologic process out of balance
PATHOPHYSIOLOGY • < 20 weeks of POG • Anabolic phase • Increase in Insulin sensitivity • > 20 weeks of POG • Catabolic phase • Increase in Insulin resistance
Pathophysiology • Early in pregnancy, maternal estrogen and progesterone increase and promote pancreatic ß-cell hyperplasia and increased insulin release • As pregnancy progresses, increased levels of human placental lactogen, cortisol, prolactin, progesterone, and estrogen lead to insulin resistancein peripheral tissues. • Table 1 describes the diabetogenic potency and time of peak effect of these hormones. The timing of these hormonal events is important in regard to scheduling testing for GDM
GDM results when there is delayed or insufficient insulin secretion in the presence of increasing peripheral resistance
Discussion • What are the risk factors for gestational diabetes? • What risk factors do you see most often in your setting?
Risk factors for GDM Low risk • High risk • Obesity • Diabetes in 1st degree relative • Previous • history of GDM or glucose intolerance • complicated pregnancy • infant with macrosomia > 3.5 kg • Older age • High risk ethnic group; South Asian, East Asian, Indigenous American or Australian, Hispanic • PCOS • Age less than 25 years • No previous poor pregnancy outcomes • No diabetes in 1st degree relatives • Normal prepregnancy weight and weight gain during pregnancy • No history of abnormal glucose tolerance Perkins, Dunn, Jagastia, 2007
Is Hypertension a risk factor? • Hypertension prior to pregnancy or during 1st trimester – doubled the risk of GDM – independent of maternal weight • Hence all women with hypertension should be screened for GDM Hedderson, Ferrara, 2008
Why diagnose and treat GDM? • Short term risks for the mother • Development of gestational hypertension, worsening essential hypertension or development of preeclampsia • Operative delivery - related to macrosomia • Polyhydramnios • Premature labour • Long term risks for the mother • Development of type 2 diabetes in next ~10 years (30-60% depending on population) • Development of cardiovascular disease CDA, 2013 Metzger, Buchanan, et al. 2007
Why diagnose and treat GDM? • Short term risks for the baby • Macrosomia • Neonatal hypoglycemia • Jaundice • Preterm birth • Birth injury • Hypocalcemia/ hypomagnesimia • Respiratory distress syndrome • Long term risks for the baby • Obesity • Type 2 diabetes
Screening • Whom to screen • When to screen • How to screen
Venous or capillary • The venous plasma is the gold standard • Where laboratory facilities or technicians are not available, capillary glucose estimations may be done using a hand held glucose meter. • The glucose meter must be standardized with a lab and calibrated against the lab on a regular basis.
Screening for GDM • Indians fall into the high-risk category for developing GDM • therefore universal screeningis recommended in pregnancy
When ?? • offer universal screening – to ALL antenatal • women at 24 – 28 wks of gestation • and an early screening at booking if there • are additional risk factors identified by history o Previous unexplained loss at term o Previous baby weight > 4 kg o Previous Pregnancy with GDM o Strong F/H
Diagnosis of Diabetes in non-pregnant women & menOGTT is not recommended for routine clinical use.The FPG is the preferred test to diagnose diabetes in children & non-pregnant adults.Use of the A1C for the diagnosis of diabetes is not recommended at this time. ADA recommendations. American Diabetes Association Criteria for Glycemic abnormalities
When to screen to rule out unidentified pre-existing diabetes?First trimester • Screening in 1st trimester • Fasting plasma glucose >126 mg/dl (7 mmol/L) • or • HbA1c >6.5% • or • Random >200mg/dl (11.1 mmol/L) • or • 2hr value in OGTT >200mg/dl (11.1 mmol/L) • If overt diabetes is detected, it must be treated appropriately. ADA, 2015
Fasting and & postprandial venous plasma sugar during pregnancy
When to screen for GDM?24-28 Weeks (One Step Strategy) • Screening should be done at 24-28 weeks • Diagnosis based on a 75 gm glucose load given in fasting state • GDM diagnosed when one or more of the following is present • Fasting 92 - 125 mg/dl (5.0 – 6.9 mmol/L) • 1 hour post 75 gm load >180 mg/dl (10 mmol/L) • 2 hour post 75 gm load >153mg/dl (8.5 mmol/L) • If woman tests negative, screening at 32 weeks also may be necessary in presence of high risks World Health Organization, 2013
DIAGNOSIS • TWO-STEP STRAREGY • 50-75g oral glucose challenge • Single serum glucose measurement @ 1 hr • <7.8 mmol/L(<140mg/dL) normal • >7.8 mmol/L(>140mg/dL) • 100-g oral glucose challenge • Serum glucose measurements in fasting state, I, II & III hrs • Normal values • Fasting < 5.8 mmol/L (<105mg/dL) • I hr < 10.5 mmol/L (<190mg/dL ) • II hr < 9.1 mmol/L (<165mg/dL) • III hr < 8.0 mmol/L (<145mg/dL)
Interesting, right? This is just a sneak preview of the full presentation. We hope you like it! To see the rest of it, just click here to view it in full on PowerShow.com. Then, if you’d like, you can also log in to PowerShow.com to download the entire presentation for free.