Download
1 / 106
1.23k likes | 1.92k Views
LASIK & PRK: Potential Post-op Corneal Opacities. Terrence S. Spencer, M.D. February, 2013. Disclosures. financial disclosure: No current financial interest or consulting fees related to any products discussed. Purpose. To educate optometrists

E N D
LASIK & PRK: Potential Post-op Corneal Opacities Terrence S. Spencer, M.D. February, 2013
Disclosures • financial disclosure: • No current financial interest or consulting fees related to any products discussed Purpose • To educate optometrists • Familiarize with possible post-operative complications of LASIK and PRK • LASIK is a surgery, and all surgery has some risk Terrence S. Spencer, M.D.
Outline • Briefly Review Corneal anatomy • Refractive Surgery vs. Corneal refractive surgery • History of Refractive Surgery • Basics of corneal refractive surgery • PRK and LASIK • Flap creating technology - Intralase. • Complications and what to do.
Corneal Anatomy • Corneal Transparency: • Based on highly organized system • Stroma: • Layers of fibroblasts between sheets of lamella. • Ground substance: • Maintain proper position of the fibrils equidistant from each other • Opacity (or scar): • Forms when organization of structure is disrupted
What is Refractive Surgery • Photo-Refractive Keratectomy • LASIK • CK: conductive keratoplasty • Phakic IOL’s – VisianStaar ICL • Refractive lens exchange or cataract surgery • Presbyopia-correcting & Toric IOLs • Corneal implants • Intracor procedure
History of Refractive Surgery • Ancient Chinese: • Slept with sandbags on eyes to flatten the cornea • 1800 -1900’s: • A variety of devices to modify the shape of cornea with pressure or suction • 1898: • keratotomy experiment in rabbits.
History of Refractive Surgery • SvyatoslavFyodorov (Moscow) • 1939-2000 • Early1970s: boy on bicycle (-6 D) • 1974: started doing RK on humans • Radial incisions “relax” tension on peripheral cornea to flatten the center • Late 1970s: US surgeons started performing RK
History of Refractive Surgery • Conveyer operating theater in Soviet Union
History of Refractive Surgery • Jose Barraquer • 1916-1998 • The father of modern refractive surgery • Several inventions • Born in Spain, but moved to Bogotá, Columbia in 1965
History of Refractive Surgery • Keratomileusis (Jose Barraquer) • 1949: 1st publication on changing shape of cornea to change refraction • Cryolathe • Layer of cornea removed • Stained and Frozen • Lathed • Sutured back in place • Sutures removed weeks later
History of Refractive Surgery • Microkeratome: (Barraquer) • Allowed for in situ correction • ALK: Automated LamellerKeratoplasty (Luis Ruis) • Microkeratome 1st makes an incomplete flap • Microkeratome readjusted for the power cut. • Never gained great popularity
History of Refractive Surgery • Laser: Light Amplification by Stimulated Emission of Radiation • 1917: theorized by Albert Einstein • 1960: first successful laser
History of Refractive Surgery • Laser: Wavelength of light is determined by the type of gas or solid medium • Example: YAG laser – crystal of Yttrium-Aluminum-Garnet = 1064 nm
History of Refractive Surgery • Excimer (Excited Dimer of Argon and Flourine) Laser: • 1968: Excimer laser invented • 1970’s: Etching silicone computer chips • 1982: RangaswamySrinivasin (IBM): excimer laser can ablate tissue without causing heat damage • 1983: Steven Trokel (NYC) patented excimer laser use for vision correction • 193 nm (ultraviolet)
History of Refractive Surgery • Photorefractive keratectomy (PRK) • 1st eye surgery done with excimer laser • 1987 in Berlin: Dr. Theo Seiler
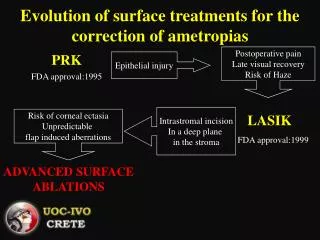
History of Refractive Surgery • 1990: Laser In-Situ Keratomeleusis (LASIK) • Epithelium intact = less pain from exposed nerves • Combines flap (ALK) with excimer laser (PRK)
PRK • PhotoRefractive Keratectomy • First performed in 1987 • Removal of tissue with excimer laser • Other names for PRK • LASEK (laser epithelial keratomileusis) • The epithelium layer is placed back on the stroma after corrective laser is completed • Epi-LASIK • A device called an epikeratome is used to remove the epithelium
Photorefractive Keratectomy (PRK) • Step 1: • Epithelium is removed • diluted alcohol, brush, vibrating blade, laser • Discarded or replaced • Step 2: • Excimer laser correction • sculpting the cornea • Either flattening or a steepening pattern +/- astigmatism correction
PRK post-op expectations • Soft bandage contact lens • Placed immediately following treatment • Helps with patient comfort • Acts as a protective barrier for the healing process • Epithelium closes in ~ 3-7 days • Epithelial healing line • Visible where leading edges of epithelium meet in center of cornea • Can induce temporary astigmatism. It can takes weeks to months to stabilize.
LASIK- laser assisted in-situ keratomileusis • Laser-Assisted • The removal of tissue is done with excimer laser • In-Situ (latin) • In place in the body • Keratomileusis • Kerato (Greek): cornea • Mileusis: to shape
LASIK SURGERY BASICS • TWO STEPS OF LASIK • 1: Corneal flap • Microkeratome or Femtosecond laser. • Layer includes epithelium, Bowman’s membrane, some anterior stroma. • The corneal flap is then folded back. • 2: Excimer laser • Ablates the corneal stroma to correct the refractive error.
LASIK SURGERY BASICS • After excimer laser treatment • Cornea irrigated with sterile saline • Examine for any debris • Irrigate until the interface is clear of any debris. • Flap is positioned back into the original position in the corneal bed • Smooth out any micro-striae
LASIK • Immediately after LASIK surgery: • Patient’s vision is foggy • cornea edema may cause difficulty to see any striae, debris etc. • Some small particles in the flap interface are not visible until the one-day post-op visit.
Concerns with LASIK • Microkeratome: • Flap creation with a blade is responsible for the majority of the possible procedural complications
What is femtosecond laser? • Femto- is a prefix in the metric system • Denotes a factor of 10-15 (0.000000000000001) • Femtosecond = 1 quadrillionth of a second • Category: ultrashort pulse (ultrafast) laser
Femtosecond laser • Advantage of ultra-short pulse lasers • Extremely precise • Cuts material by ionizing it at the atomic level • Pulses are too brief to transfer heat to the material being cut • No damage to surrounding tissue • Femtosecond lasers are “cold” lasers
The IntraLase®laser is a femtosecondlaser • How does a laser cut a flap?
Femtosecond Laser • Laser pulse is focused to desired corneal depth • Depth and hinge placement are adjustable based on individual patient factors • Corneal thickness, steepness, and/or diameter • FS laser produces precisely beveled edge architecture to enable secure flap positioning • Resists displacement • Less risk of epithelial ingrowth.
1 Micron A microplasma is created, vaporizing approximately 1 micron of corneal tissue IntraLase Photodisruption A pulse of laser energy is focused to a precise spot inside the cornea
2 Microns IntraLase Photodisruption An expanding bubble of gas & water is createdseparating the corneal lamellae
IntraLase Photodisruption The bi-products of photodisruption (CO2 & water) are absorbed by the mechanism of the endothelial pump, leaving a cleavage plane in the cornea
IntralasePhotodisruption Tighter spot placement facilitates easier flap lifts
IntraLase Photodisruptionto create horizontal cleavage plane
The Planar Flap • IntraLase provides uniform flap thickness • Independent of patient keratometry • Reduction of induced irregular astigmatism • Optimizes stromal bed for wavefront guided vision correction • Increased flap stability (less slipped flaps)
Intralase • Contraindicated in eyes with a corneal scar. • Laser may not penetrate through the opacity • May cause a gas bubble breakthrough or a tear in the flap underneath the scar
Differential Diagnosis 1)Superficial PunctateKeratitis (SPK) 2)Diffuse Lamellar Keratitis (DLK) 3)Epithelial ingrowth 4)Interface debris • Tear film –oily deposits • Cloth fiber • Cilia, Eyelash • Sponge particles • Mascara • Etc
Differential Diagnosis Cont. 5)Corneal infiltrate 6)Corneal ulcer 7)Herpetic lesion 8)Epithelial Basement Membrane Dystrophy (EBMD) 9)Micro striae vs. Slippped flap or folds 10)Prominent corneal nerves