Download
1 / 33
330 likes | 557 Views
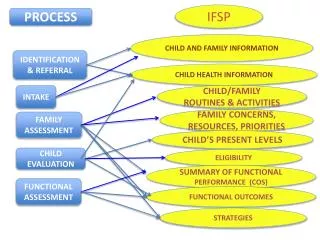
Timely Identification and Referral of Potential Organ Donors. Paul Murphy National Clinical Lead for Organ Donation. Objectives. To understand the current difficulties with donor identification and referral

E N D
Timely Identification and Referral of Potential Organ Donors Paul Murphy National Clinical Lead for Organ Donation Midlands Collaborative, November 2012
Objectives • To understand the current difficulties with donor identification and referral • To recognise the benefits of improving current elements of the identification and referral processes • Proportion of potential donors identified and referred • Timeliness of referral • Responsiveness to referral • To agree to adopt one or other of the proposed methods of identification and referral • Collaboration between SN-OD teams and referring hospitals • To understand implementation and monitoring programme Midlands Collaborative, November 2012
Outline • Data • Donation after Brain Death • Donation after Circulatory Death • Timings of donation pathway • Existing identification and referral criteria • New guidance • Provenance • Potential benefits • Key features • Options • Implementation and monitoring Midlands Collaborative, November 2012
= one (or more) Trust/Health Board Referral rates for potential DBD donors, 2010/11 99.8% CL 95% CL National rate 95% CL 99.8% CL Midlands Collaborative, November 2012
= one (or more) Trust/Health Board Referral rates for potential DCD donors, 2010/11 99.8% CL 95% CL National rate 95% CL 99.8% CL Midlands Collaborative, November 2012
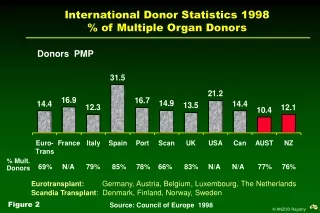
UK rates of referral Midlands Collaborative, November 2012
Progression through the donation pathway Midlands Collaborative, November 2012
SN-OD responsiveness Midlands Collaborative, November 2012
Referral to attendanceVariation across UK Midlands Collaborative, November 2012
Overall timings Midlands Collaborative, November 2012
General Medical Council, 2010 If a patient is close to death and their views cannot be determined, you should be prepared to explore with those close to them whether they had expressed any views about organ or tissue donation, if donation is likely to be a possibility. You should follow any national procedures for identifying potential organ donors and, in appropriate cases, for notifying the local transplant coordinator. Decisions to limit or withdraw treatments in potential DCD donors MUST be in compliance with national End of Life Care policy. Midlands Collaborative, November 2012
ODTF Minimum notification criteria Donation after Brain-stem Death When no further treatment options are available or appropriate, and there is a plan to confirm death by neurological criteria, the DTC should be notified as soon as sedation/analgesia is discontinued, or immediately if the patient has never received sedation/analgesia. This notification should take place even if the attending clinical staff believe that donation (after death has been confirmed by neurological criteria) might be contra-indicated or inappropriate. Midlands Collaborative, November 2012
ODTF Minimum notification criteria Donation after Circulatory Death In the context of a catastrophic neurological injury, when no further treatment options are available or appropriate and there is no intention to confirm death by neurological criteria, the DTC should be notified when a decision has been made by a consultant to withdraw active treatment and this has been recorded in a dated, timed and signed entry in the case notes. This notification should take place even if the attending clinical staff believe that death cannot be diagnosed by neurological criteria, or that donation after cardiac death might be contra-indicated or inappropriate. Midlands Collaborative, November 2012
UK Donation Ethics Committee There is no ethical dilemma if the treating clinician wishes to make contact with the SN-OD at an early stage, while the patient is seriously ill and death is likely, but before a formal decision has been made to withdraw life-sustaining treatment. [Benefits] include establishing whether there are contra-indications for organ donation…… Other practical and organisational factors might be relevant – if the SN-OD is based at a distant location then early contact can help to minimise distressing delays for the family. Midlands Collaborative, November 2012
British Medical Association, 2012 The research data analysed by NICE showed that the use of clinical triggers and a requirement to refer according to standard criteria led to an increase in both referrals and donors. It is hoped that implementation of the NICE guideline will result in early and consistent donor referral. Midlands Collaborative, November 2012
NICE SCG 135 Midlands Collaborative, November 2012
Donor Assessment Midlands Collaborative, November 2012
NHS BT Strategy • Implementation not publication • Key area for collaboration between hospitals and donor care teams • Very clear emphasis on benefits • How not who • Suite of options • Clarity over implementation Midlands Collaborative, November 2012
Problems • Not all patients are referred • DCD • Not all patients are referred as early as they might be • Intention to test • Clinical triggers • SN-OD response times are not always as we would like them • Geographical deployment Midlands Collaborative, November 2012
Provenance Midlands Collaborative, November 2012
Objectives, benefits and outcomes All potential donors are identified and referred All patients are given the option of donation Access to clinical advice Prompt donor optimisation Resolution of potential legal obstacles Early assessment of marginal donors Early tissue typing / screening Planning the family approach Reduction in delays for families and units All donors are referred in a timely fashion SN-ODs are deployed in a way that improves responsiveness Increased donor numbers Improved consent / authorisation rates Increase in donor organs Better experience Midlands Collaborative, November 2012
Planning the family approach Planning Establish the team: Consultant, SN-OD and nurse Clarify clinical situation Seek evidence of prior consent Key family members by name Key family issues Agree a process of approach and who will be involved Agree timing and setting, ensuring these are appropriate to family needs Involve others as required, eg faith leaders Confirming understanding and acceptance of loss Discussing donation Midlands Collaborative, November 2012
Strategy proposals Donation Committees and SN-OD teams are asked to collaborate to develop and implement a policy that ensures that all potential donors are identified and referred in a timely fashion. • Every hospital should have a written policy for the identification and timely referral of all potential donors • As a minimum every donating area within a given hospital adopts a consistent approach • In circumstances where clinicians feel conflicted, consider approaches that ‘decouple’ early referral from that clinician Midlands Collaborative, November 2012
1. Daily visit by SN-OD Midlands Collaborative, November 2012
2. Early daily phone call Midlands Collaborative, November 2012
3. Daily ICU team safety brief Midlands Collaborative, November 2012
Frenchay ICU team safety brief Midlands Collaborative, November 2012
Frenchay ICU team safety brief Midlands Collaborative, November 2012
4. Standard Operating Procedure Midlands Collaborative, November 2012
Midlands Standard Operating Procedure Midlands Collaborative, November 2012
Midlands Standard Operating Procedure Midlands Collaborative, November 2012
5. Nurse led referrals Midlands Collaborative, November 2012
Implementation • All hospitals to adopt a referral strategy by 31 January 2013 • SN-ODs to be present at an appropriate time at least five days per week on the ICUs of all level 1 hospitals • Non referrals continue to be reported by the PDA • Next update of PDA will examine the timeliness of referral • SN-OD teams will be managed against their responsiveness Midlands Collaborative, November 2012
![Assessing Potential Altruistic [Non-Directed] Living Organ Donors](https://cdn1.slideserve.com/1708861/assessing-potential-altruistic-non-directed-living-organ-donors-dt.jpg)