Download

1 / 39
0 likes | 9 Views
Jail Triage is a voluntary program in Kentucky's county jails aimed at screening for suicide risk, managing mental health crises, and reducing the likelihood of custodial suicides. The program involves identifying at-risk inmates, recommending interventions, and collaborating with local mental health services. Operational objectives include proper restraint, timely observation, and reasonable provision of suicide risk management. Various risk indicators are considered, such as inmate responses at booking, institutional alerts, observations of behavior, and information provided by multiple sources. Substance-related concerns, withdrawal symptoms, and specific risk factors are also addressed to ensure comprehensive care and reduce harm within correctional facilities.

E N D

Jail Triage Program Goals Jail Triage is a voluntary program available to Kentucky’s county jails that screens for suicide risk, recommends interventions and arranges follow-up assessments with local mental health as needed. Its goals focus on: Lessening the likelihood of custodial suicide. Helping jails manage mental health crises.
Jail Triage Objectives Identify inmates at risk for suicide. Identify inmates with serious mental illness. Make recommendations to the jail for managing these risks.
Jails’ Operational Objectives Proper restraint and housing Timely observation and documentation Timely and reasonable provision of suicide risk management
Operational Failures Knowledge of a behavioral health risk Understanding the consequences of the risk Wanton or intentional failure to reasonably avoid the risk Resulting harm from the failure

Identifying Risk Jail staff identify possible risk through: Inmate responses to screening questions at booking. Institutional alerts from past incarcerations. Observations of behavior at the jail. Information provided by arresting or transporting officers, or transferring agencies. Information provided by third parties: friends, family, hospitals, attorneys, court staff, other inmates, etc.

Free to Participating Jails Once a potential risk for suicide or mental health crisis has been identified, the jail calls: 877-266-2602
Triage Assessment A Jail Triage clinician will return the jail’s call to gather further information and determine: Level of risk: Critical, High, Moderate, Low Recommended jail protocols Follow-up requirements
When to Triage Any time suicide or mental health concerns arise: At intake At booking/screening When there are institutional alerts When there is event-driven risk When there is observation of risk
At Intake When the arresting or transporting officer responds to Jail Intake Assessment questions and reports: Arrestee made statements of self harm Family or friends warned of statements or actions indicating self harm Arrestee’s reaction to arrest suggested risk of self harm Arrestee’s behaviors suggested mental illness
At Booking/Screening Arrestee reports prior suicide attempts Arrestee reports current suicidal ideation Arrestee reports hospitalization for mental illness in the past year Arrestee reports a serious mental health condition
Institutional Alerts Arrestee was triaged at critical or high risk level during a past incarceration for: Suicide risk or self harm Acute symptoms of mental illness Substance-induced risk factors Behavioral risk factors Arrestee was designated during a past incarceration as having an intellectual or developmental disability, serious mental illness or brain injury.
Event-Driven Risk Severity of charge or length of sentence Upsetting court appearance or news about case Response to disciplinary action Bad phone call or visit Death of loved one
Observation of Risk Another inmate expresses concern about self- harm or mental instability Jail staff observe overt signs of depression, psychosis or other acute distress Jail staff discover preparations for self-harm or observe active efforts to harm self Family or another third party contacts the jail to express concern
Overt Indications of Distress Making instruments of suicide: noose, shank, hoarding medication Engaging in self-injury: cutting, scratching, head-banging Refusing meals, medication Terminating communication: letters, phone calls, visits Declining showers, recreation, commissary Saying goodbye, giving away property, preparing will Exhibiting significant emotional upset, physical agitation, or withdrawal including requests for segregation
Substance-related Concerns Substance use can heighten suicide risk factors by Decreasing inhibitions Increasing psychological distress Increasing aggressiveness Constricting cognition so the person can’t see beyond their current despair The Substance Abuse & Mental Health Services Administration reports that Suicide is the leading cause of death among people who misuse alcohol and drugs. A large percentage of suicides had substances in their system at time of death: 22% alcohol, 20% opiates, 10.2% marijuana, 4.6% cocaine, and 3.4% amphetamines. The presentation of someone impaired or withdrawing from substances can be easily confused with mental health problems and not be recognized as a potential medical emergency.
Withdrawal Symptoms Always refer arrestees to medical staff if there is any indication of substance use. Medical clearance at the local hospital before taking custody may guard against overdose, but withdrawal can also be deadly. It may be days before serious symptoms appear. Be particularly mindful of inmates withdrawing from these substances: Alcohol Benzodiazepines Opiates Even if the inmate did not disclose withdrawal risk, symptoms listed on the following pages can indicate need for immediate medical attention.

Alcohol Withdrawal Seizures and delirium tremens (DTs) are the most serious alcohol withdrawal symptoms and can result in death. Watch for these symptoms: shaking, shivering, irregular/fast heartbeat, high blood pressure, heavy sweating, hallucinations, very high fever, nightmares, global confusion, and seizures. Can occur up to 3 days into withdrawal. More likely among inmates who have had a high intake of alcohol for more than one month (7-8 pints of beer daily or 1 pint of liquor daily). History of seizures/DTs predicts future withdrawal episodes.

Benzodiazepine Withdrawal Catatonia, convulsions/seizures, delirium tremens (DTs) similar to alcohol withdrawal and increased suicidal ideation are the most serious benzodiazepine withdrawal symptoms and can result in death. Watch for these symptoms: psychosis, confusion, fever, mania, aggression, and psychomotor rigidity or severe psychomotor agitation. Can occur within 6-8 hours for short-acting benzodiazepines. Can occur within 24-48 hours for long-acting benzodiazepines. Closely monitor on days 3 and 4. Fatal symptoms often manifest during this window for heavy benzodiazepine users.

Opiate Withdrawal Complications from persistent vomiting and diarrhea are the most serious opiate withdrawal symptoms and can result in death. Dehydration and elevated sodium levels may result in heart failure. Inadvertently breathing vomited material into the lungs may result in suffocation. Watch for these dehydration symptoms: dizziness/fainting, rapid heartbeat and breathing, confusion/irritability, decreased urine output/dark colored urine, fatigue/sleepiness, and low blood pressure. Symptoms for short-acting opiates (heroin) peak at around 2-3 days. Symptoms can continue for up to 10 days.
Withdrawal Emergencies The withdrawal symptoms listed on the previous slides indicate a medical emergency. Seek immediate help from a medical professional, whether that be the jail’s own medical staff or an ambulance. Even if the inmate didn’t acknowledge using these substances, the symptoms are just as life-threatening. Trust observable symptoms over self- report. Remember: People struggling with addiction routinely downplay the extent of their use. Inmates may be reluctant to acknowledge use that they believe could impact their case. Drugs are often cut with substances unknown to the user.

The Jail Triage Process When the arrestee is triaged, jail staff will be asked to provide basic information from all available sources such as: Name, SSN, DOB, charges noting felonies, booking date, known substances in use, withdrawal potential, any flags they had a booking The concern that prompted the call to Jail Triage Any past institutional alerts Current inmate presentation
Risk Leveling Critical High Moderate Low

Critical Risk Level Active suicide attempts Other active self-injurious behaviors
High Risk Level Active suicidal thoughts History of suicide attempts less than 2 years ago Concern related to charge-related risk Agitated psychosis Lower level risk compounded by such things as substance use that jeopardizes inmate’s immediate safety
Moderate Risk Level History of suicide attempts between 2 and 10 years ago Family history of completed suicide Significant mental health treatment history or potential medication issues at the jail Psychiatric hospitalization in the last year Active emotional distress without suicide ideation Lower level risk compounded by added risk factors
Low Risk Level Suicide history of attempts more than 10 years ago Minor mental health history Absence of other compounding risk factors
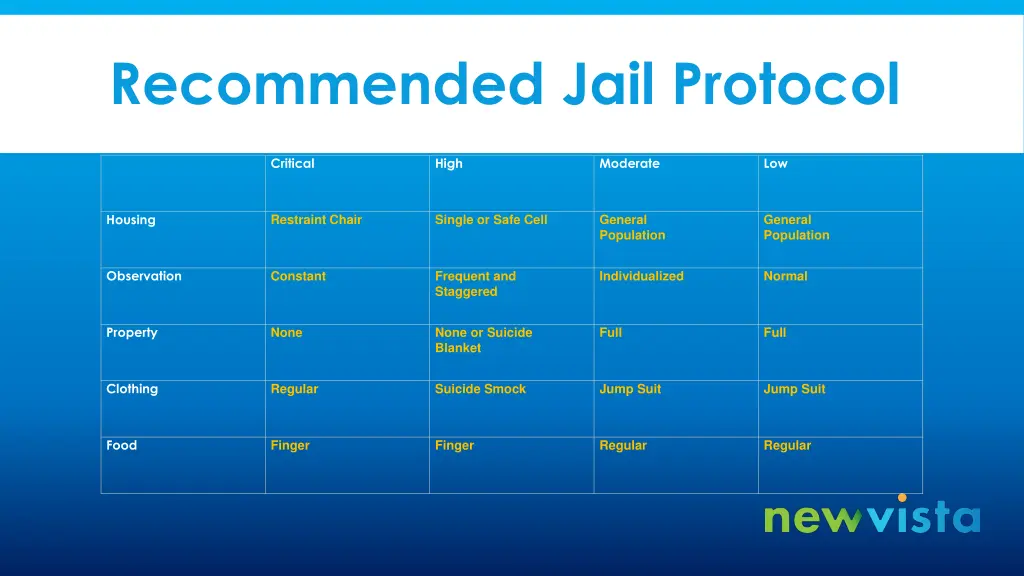
Recommended Jail Protocol Critical High Moderate Low Housing Restraint Chair Single or Safe Cell General Population General Population Observation Constant Frequent and Staggered Individualized Normal Property None None or Suicide Blanket Full Full Clothing Regular Suicide Smock Jump Suit Jump Suit Food Finger Finger Regular Regular
Kingsley v. Hendrickson Any force used to prevent suicide or injury must be objectively reasonable. For example: Using a safety chair to prevent an active suicide attempt is preferable to forced clothing removal for subsequent placement in a suicide smock It is reasoned that the safety chair is less traumatic than a forced clothing removal Placement in a safety chair after clothing removal in a smock further traumatizes the inmate as the smock often fails to cover genitals and is often recorded.

Clinician Recommendations Once a risk level has been assigned, it will be accompanied by one of these three recommendations: Maintain risk level pending contact with mental health within a specified timeframe. Maintain risk level for a specified timeframe and then call Jail Triage to retriage. Maintain the risk level for a specified period of time and then reduce to the next lower level if no concerns arise.

Fail Safe Regardless of Triage recommendation, when in doubt or if you have any questions call: Jail Triage 877-266-2602

Mental Health Follow-Up Jail Triage may recommend contact with local mental health for further suicide assessment. This follow-up may be conducted by phone, by video or in person depending on your local provider’s procedures for this. Jail staff will be responsible for making the inmate available once mental health contacts the jail to assess inmate. In the event of inmate refusal or safety concerns regarding this contact, the risk level will be maintained and a retriage will be recommended for a later time. In addition to leveling recommendations, mental health may suggest such things as involuntary hospitalization, use of inmate watchers, referrals to jail medical staff or EMT, the chaplain, internal mental health staff or ongoing mental health treatment options. Using Jail Triage does not preclude contracting with another mental health provider for additional services as jail administration sees fit.
Retriage If a retriage is recommended, jail staff initiates this by calling Jail Triage after the recommended timeframe. Jail staff should be prepared with all documentation to date on inmate, including recommendations made after any assessments by local mental health. Jail staff will also be asked if inmate is reporting thoughts of suicide or other distress, about inmate’s current presentation, and about any changes in status since the last triage or assessment. Jail Triage staff will use this information to reassess inmate’s risk level and make recommendations accordingly.
202a Commitments 202a assessments for involuntary psychiatric hospitalizations are provided through state contracts with the local mental health agency serving that judicial district. Jail Triage cannot initiate a 202a petition or perform the assessment but can provide collateral Jail Triage information to the local mental health provider if requested. If the jail receives a 202a petition or initiates paperwork for a 202a assessment, the appropriate contact is the local mental health provider.
Jail Triage Limitations The legal jurisdiction of Jail Triage begins when custody is accepted and ends upon legal release or custody transfer from the holding jail. Risk leveling by Jail Triage applies to in-custody assessments and not to community release. Any inmate being released from the jail on a high or critical risk leveling status should be advised to seek community mental health services. The jail should also consider providing: A 202a referral A call to the inmate’s emergency contact number A business card with the community mental health contact information or number for the community mental health crisis line.
Community MH Crisis Line Numbers Adanta – 800-633-5599 Centerstone – 800-221-0446 Communicare – 800-641-4673 Comprehend – 877-852-1523 Cumberland River – (day) 606-864-2104 (afterhours) 800-273-8255 Four Rivers – 800-592-3980 Kentucky River – 800-262-7491 LifeSkills – 800-223-8913 Mountain Comp – 800-422-1060 New Vista – 800-928-8000 NorthKey – 877-331-3292 Pathways – 800-562-8909 Pennyroyal – 877-473-7766 River Valley – 800-433-7291
Community Engagement As the jail assumes a duty to protect inmates from suicide, it is prudent to engage an inmate’s family, friends and professional associates in suicide prevention. Signage and phone messaging should advise significant others of their responsibility to notify the jail staff of any inmate action or communication that threatens the safety of an inmate. We all share the responsibility to prevent harm to those in custody.

Mental Health Jail Training The state requires 4 hours of mental health training for jail personnel during the first year of service. One hour of mental health training is required for each year thereafter. Jail Triage is willing to provide this training for a fee. Jail Triage online training materials are available at www.newvista.org. Click the Jail Triage link at the bottom of the home page.

![[PDF] Free Download The Fifth Risk By Michael Lewis](https://cdn4.slideserve.com/8030539/slide1-dt.jpg)