Download
1 / 37
370 likes | 566 Views
TB new treatments and new methodological challenges. Dr Corinne Merle. Outline. C urrent pipeline of new TB drugs Methodological challenges for designing TB trials (using the OFLOTUB project as an example) Challenges in TB regimen development. TB drug development: to set the scene.

E N D
TB new treatments and new methodological challenges Dr Corinne Merle
Outline • Current pipeline of new TB drugs • Methodological challenges for designing TB trials (using the OFLOTUB project as an example) • Challenges in TB regimen development
TB drug development: to set the scene 1961 Ethambutol (E) 1952 Isoniazid (H) 1963 Rifampicin (R) 1943 Streptomycine (S) 1954 Pyrazinamide (Z) 1882 1940 1950 1960 1970 1980 1990 2000 2010 Description of the agent of TB 1970s: short course regimen: S/H/R or S/H/Z -9 months therapy 1946: 1st drug: S Montotherapy led to S resistance 1952: 1st regimen: S/PAS/H 18-24 months therapy 1980s: modern short-course regimen: E (S) H R Z 6 months of therapy
TB drug development: to set the scene • Effective treatment: 95% of treatment efficacy • But... • 6 months treatment regimen • problem of treatment adherence • Emergence of MDRTB • 8.8 millions new TB cases in 2010 1961 Ethambutol (E) 1952 Isoniazid (H) 1963 Rifampicin (R) 1943 Streptomycine (S) 1954 Pyrazinamide (Z) 1882 1940 1950 1960 1970 1980 1990 2000 2010 Description of the agent of TB 1970s: short course regimen: S/H/R or S/H/Z -9 months therapy 1946: 1st drug: S Montotherapy led to S resistance 1952: 1st regimen: S/PAS/H 18-24 months therapy 1980s: modern short-course regimen: E (S) H R Z 6 months of therapy
Development pipeline for new TB drugs • Shortening TB treatment recognised as a major target for the improvement of TB control • Since the late 90s: new agents discovered • Significant target diversity and potential for better combinations
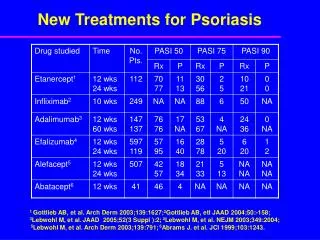
Drugs at a Phase III stage • Both gatifloxacin and moxifloxacin have emerged as candidates from the 8-methoxyfluoroquinolones drug class and are proposed for shortened treatment of pan-susceptible TB. • Gatifloxacin was chosen based on its bactericidal activity and its generic status • 35 years after the East African/British Medical Research Council trials, 3 new drugs currently assessed in large Phase III trials • RIFAQUINtrial (Rifapentine) • REMoxTB trial (Moxifloxacin) • OFLOTUB trial (Gatifloxacin) flotub
Gatifloxacin Product Development Plan • Pre-Clinical Toxicology studies • Phase I Pharmacokinetic study(J AntimicrobChemother. 2007 Dec;60(6):1398-401) • Phase II SSCC study (Int J Tuberc Lung Dis. 2008 Feb;12(2):128-38. ). • Phase III pivotal trial with a nested PK/PD also called OFLOTUB More than 10 years in development flotub
Overview of OFLOTUB project: Phase III/PK • Objective To evaluate the efficacy and safety of 4-month gatifloxacin containing regimen compared to the standard WHO-recommended 6-month regimen • Study design A randomized (1:1), open-label, non-inferiority, multi-centre controlled trial with a nested Pharmacokinetic (PK/PD) study • Patients Newly diagnosed microbiologically confirmed TB sensitive adults patients in 5 countries in Africa flotub
Overview of OFLOTUB project: Phase III/PK • Treatment • Test arm : 2 months GHRZ / 2 months GHR • Control arm: 2 months EHRZ / 4 months RH • Daily DOT during the 1st 2 months of treatment, • Weekly drug deliveryduring the continuation phase • Follow-up • 2 years after completion of TB treatment • Patients seen at 1, 2, 4, 6, 9, 12, 15, 18 and 24 months after treatment • Clinical examination, 2 sputum samples collected for smear & culture flotub
Trial setting and OFLOTUBpartners Tropical Medical Institute (Antwerp) Hôpital Raymond Poincaré (Paris) LUPIN Pharma (India) St George’sHospitalMedical School, (London) WHO / TDR (Geneva) Thamassat University (Bangkok) Institute for Research & Development(Marseille) PNLTB (Dakar, Senegal) KEMRI (Nairobi, Kenya) PNLTB (Conakry, Guinea) PNLTB (Cotonou, Benin) MRC SA (Durban, South Africa) London School of Hygiene and Tropical Medicine (London) flotub
Trial setting and OFLOTUBpartners Tropical Medical Institute (Antwerp) Hôpital Raymond Poincaré (Paris) LUPIN Pharma (India) St George’sHospitalMedical School, (London) WHO / TDR (Geneva) Thamassat University (Bangkok) Institute for Research & Development(Marseille) PNLTB (Dakar, Senegal) KEMRI (Nairobi, Kenya) PNLTB (Conakry, Guinea) PNLTB (Cotonou, Benin) MRC SA (Durban, South Africa) London School of Hygiene and Tropical Medicine (London) flotub
Trial setting and OFLOTUBpartners Tropical Medical Institute (Antwerp) Hôpital Raymond Poincaré (Paris) St George’sHospitalMedical School, (London) WHO / TDR (Geneva) Thamassat University (Bangkok) Institute for Research & Development(Marseille) PNLTB (Dakar, Senegal) KEMRI (Nairobi, Kenya) PNLTB (Conakry, Guinea) PNLTB (Cotonou, Benin) MRC SA (Durban, South Africa) London School of Hygiene and Tropical Medicine (London) LUPIN Pharma (India) flotub
Trial setting and OFLOTUBpartners Tropical Medical Institute (Antwerp) Hôpital Raymond Poincaré (Paris) St George’sHospitalMedical School, (London) WHO / TDR (Geneva) Thamassat University (Bangkok) Institute for Research & Development(Marseille) PNLTB (Dakar, Senegal) KEMRI (Nairobi, Kenya) PNLTB (Conakry, Guinea) PNLTB (Cotonou, Benin) MRC SA (Durban, South Africa) London School of Hygiene and Tropical Medicine (London) LUPIN Pharma (India) flotub
Trial setting and OFLOTUBpartners London School of Hygiene and Tropical Medicine (London) Tropical Medical Institute (Antwerp) Hôpital Raymond Poincaré (Paris) St George’sHospitalMedical School, (London) WHO / TDR (Geneva) Thamassat University (Bangkok) Institute for Research & Development(Marseille) PNLTB (Dakar, Senegal) KEMRI (Nairobi, Kenya) PNLTB (Conakry, Guinea) PNLTB (Cotonou, Benin) MRC SA (Durban, South Africa) LUPIN Pharma (India) flotub
Overview of OFLOTUB project: Phase III/PK • Progress status • 1836 patients recruited • 316 in Benin, 452 in Guinea, 200 in Kenya, 358 in Senegal and 510 in South Africa • Last patient completed treatment end of April 2009 • Last patient last visit: April 2011 (i.e. 24 months of follow-up following the end of treatment) • Percentage of patients LTFU estimated to be around 10 % • First results should be released in November 2012
Non-inferiority design Rationale for Choice of Non-inferiority design • Highly efficient current TB treatment (95% cure rate) • Unlikely that a new regimen will demonstrate superiority • Interest lies with showing whether a new regimen is not inferior Non-inferiority design is an excellent choice for current TB sensitive drug development (A. Nunn et al, Tuberculosis(2008)) flotub
Non-inferiority design Rationale for Choice of Non-inferiority design • Highly efficient current TB treatment (95% cure rate) • Unlikely that a new regimen will demonstrate superiority • Interest lies with showing whether a new regimen is not inferior NI design is an excellent choice for current TB sensitive drug development (A. Nunn et al, Tuberculosis(2008)) • Implication of NI design on trial population to be analysed • Intention-To-Treat (ITT) Vs Per-Protocol (PP) • ITT approach tends to minimise differences by including protocol deviations • PP is biased because not including all randomised patients • In fact, both are equally important and require similar conclusions in order to support final result (Piaggio G, Elbourne DR, et al. JAMA 2006;295(10):1152-60.) flotub
Choice & measurement of the endpoints • In 1947, endpoint of BMRC Streptomycin trial: Survival or Chest Xray • Nowadays, bacteriological endpoints • TB recurrence main outcome of interest • But restricted to patients cured at the end of the treatment • A composite “unfavourable outcome” endpoint including: • - treatment failure • Death • TB recurrences flotub
Choice & measurement of the endpoints • Bacteriological diagnosis: Cultures • Solid Vs liquid media • False-positive cultures results from • Misidentification of the strain • Laboratory cross-contamination • Clerical error reporting • More than 3 % of false positive (Burman et al Clin Infect Dis 2000, 31(6):1390-1395) • Necessity to take 2 sputum samples per visit, per patient to minimise unavailability or false positive culture results • Solid medium is the gold standard
Recurrence, relapse and re-infection • Relapse : Reactivation of the original infection • Re-infection: Infection with a new TB strain • Effective treatment should prevent relapse but have no effect on re-infection • Context of TB and HIV, proportion of re-infection can be high • Non-inferiority design context Necessity to differentiate relapse from re-infection using molecular method (e.g. MIRU-VNTR) Recurrence considered to allow comparison with previous trials flotub
Length of patient follow-up • For a TB regimen to be acceptable: • Patient must convert to culture negative by the end of treatment • most importantly, it must demonstrate clearance of bacteria by keeping patients relapse-free • How long is long enough? • When to start the clock…after the end of treatment (equal follow-up between arms)? or post randomization (unequal follow-up)? • Conservative approach: 24 months after the end of the treatment • In the light of BMRC trials: 1 year follow-up could be enough • (Nunn AJ et al. Int J Tuberc Lung Dis 2010, 14(2):241-242) • Discussion on when to start the clock (even more important for shorter treatment regimen trial) flotub
Blinded design versus Open-label design Options • i) non-blinded design: an arm with 4 months of test regimen vs an arm with 6 months of standard regimen • ii) blinded design : 2-months placebo added to the test arm Discussion • Double blinding design favoured in many trial situations • For a shorter regimen, one of the mechanisms for treatment efficacy might be better adherence to treatment • Aspect not captured in blinded design • Pro and Cons Requirements if Open-label design • Laboratory staff are blinded to the treatment regimen the patient is receiving • Strict & objective endpoint definitions and a blinded endpoint committee
Sample size calculation Importance of being powered for both ITT and PP analysis
TB Drug development challenges • Objective is to get new TB treatment regimen not only new TB drug • Novel 3-drug combinations that have potential to: • Shorten treatment to 2 months or less • Be co-administered with ARVs • Be effective against MDR- and XDR-TB 24-30 Years ABCD GFE E AB • Conventional approach would need 24-30 years to develop a combination that contains ≥ 3 new drugs • Adaptive multi-arm multistage (MAMS) trial design, which has been successfully used in cancer — is under discussion. • Even if MAMS, TB drug trial are long and costly D G 8-10 years 8-10 years ABCE ABFE F C 8-10 Years
Gatifloxacin product development Length Dec 2002, Grant approval (P III) Jan - Mars 2005, initiation visits in the 5 recruitment sites for Phase III & PK/PD August 2003, Phase I & PK Phase III: April 2011, last patient FU July 2004, Phase II SSCC Phase I, Phase II, Phase III & PK/PD Design of the phase III study & set-up, capacity building +++ Phase III Recruitment period Follow-up period Nov 2012, 1st efficacy results In total 10 to 11 years Phase III: last patient recruited: 31 Oct 2008 flotub
Gatifloxacin product development Length Dec 2002, Grant approval (P III) Jan - Mars 2005, initiation visits in the 5 recruitment sites for Phase III & PK/PD August 2003, Phase I & PK Phase III: April 2011, last patient FU July 2004, Phase II SSCC Phase I, Phase II, Phase III & PK/PD Design of the phase III study & set-up, capacity building +++ Phase III Recruitment period Follow-up period Nov 2012, 1st efficacy results 2.5 years Phase III: last patient recruited: 31 Oct 2008 flotub
Gatifloxacin product development Length Dec 2002, Grant approval (P III) Jan - Mars 2005, initiation visits in the 5 recruitment sites for Phase III & PK/PD August 2003, Phase I & PK Phase III: April 2011, last patient FU July 2004, Phase II SSCC Phase I, Phase II, Phase III & PK/PD Design of the phase III study & set-up, capacity building +++ Phase III Recruitment period Follow-up period Nov 2012, 1st efficacy results 2.5 years Phase III: last patient recruited: 31 Oct 2008 flotub
Gatifloxacin product development Length Dec 2002, Grant approval (P III) Jan - Mars 2005, initiation visits in the 5 recruitment sites for Phase III & PK/PD August 2003, Phase I & PK Phase III: April 2011, last patient FU July 2004, Phase II SSCC Phase I, Phase II, Phase III & PK/PD Design of the phase III study & set-up, capacity building +++ Phase III Recruitment period Follow-up period Nov 2012, 1st efficacy results 3.5 years Phase III: last patient recruited: 31 Oct 2008 flotub
Gatifloxacin product development Length Dec 2002, Grant approval (P III) Jan - Mars 2005, initiation visits in the 5 recruitment sites for Phase III & PK/PD August 2003, Phase I & PK Phase III: April 2011, last patient FU July 2004, Phase II SSCC Phase I, Phase II, Phase III & PK/PD Design of the phase III study & set-up, capacity building +++ Phase III Recruitment period Follow-up period Nov 2012, 1st efficacy results 2 years ? Phase III: last patient recruited: 31 Oct 2008 flotub
Gatifloxacin product development Length Dec 2002, Grant approval (P III) Jan - Mars 2005, initiation visits in the 5 recruitment sites for Phase III & PK/PD August 2003, Phase I & PK Phase III: April 2011, last patient FU July 2004, Phase II SSCC Data management Phase I, Phase II, Phase III & PK/PD Design of the phase III study & set-up, capacity building +++ Phase III Recruitment period Follow-up period Nov 2012, 1st efficacy results Phase III: last patient recruited: 31 Oct 2008 flotub
To reduce the length of TB drug development • Set-up phase • Enhancing local capacity; training & re-training….. Huge capacity building investment, important that it is being capitalised and optimised • Necessity to ensure continuity of the research investments in these sites • Necessity to adopt common guidelines for designing TB treatment trials • Recruitment period • Patient follow-up & outcome of interest • Reduced to 12 months post treatment • Necessity to validate surrogate markers • Datamanagement
Conclusion • Shortening the duration of TB treatment is the majortarget • There are TB drug development challenges • There are methodological challenges when designing phase III TB sensitive RCT • We are advocating for: • a non-inferiority design, • a non-blinded design, • a composite unfavourable endpoint, • a follow-up of 12 months post treatment completion, • added trial procedures specifically aiming at minimizing unavailability of endpoints, • and distinguishing between relapse and re-infection. flotub
Conclusion 1961 Ethambutol (E) 1952 Isoniazid (H) ? 1963 Rifampicin (R) 1943 Streptomycine (S) 1954 Pyrazinamide (Z) 1882 1940 1950 1960 1970 1980 1990 2000 2010 Description of the agent of TB 1970s: short course regimen: S/H/R or S/H/Z -9 months therapy 1946: 1st drug: S Montotherapy led to S resistance 1952: 1st regimen: S/PAS/H 18-24 months therapy 1980s: modern short-course regimen: E (S) H R Z 6 months of therapy
Conclusion • TB Alliance is instrumental (www.tballiance.org) 1961 Ethambutol (E) 1952 Isoniazid (H) ? 1963 Rifampicin (R) 1943 Streptomycine (S) 1954 Pyrazinamide (Z) 1882 1940 1950 1960 1970 1980 1990 2000 2010 Description of the agent of TB 1970s: short course regimen: S/H/R or S/H/Z -9 months therapy 1946: 1st drug: S Montotherapy led to S resistance 1952: 1st regimen: S/PAS/H 18-24 months therapy 1980s: modern short-course regimen: E (S) H R Z 6 months of therapy
Conclusion • Ignoring the vulnerable • Children • TB/HIV co-infected patients 1961 Ethambutol (E) 1952 Isoniazid (H) ? 1963 Rifampicin (R) 1943 Streptomycine (S) 1954 Pyrazinamide (Z) 1882 1940 1950 1960 1970 1980 1990 2000 2010 Description of the agent of TB 1970s: short course regimen: S/H/R or S/H/Z -9 months therapy 1946: 1st drug: S Montotherapy led to S resistance 1952: 1st regimen: S/PAS/H 18-24 months therapy 1980s: modern short-course regimen: E (S) H R Z 6 months of therapy