Download
1 / 28
280 likes | 402 Views
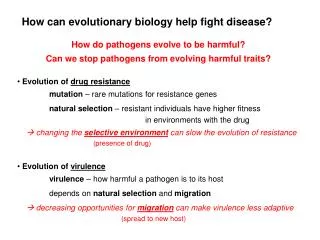
Biology of Disease CH0576. Ischaemic Heart Disease (Coronary Artery Disease). Ischaemic Heart Disease. A collective term to describe a range of conditions characterised by inability of the coronary arteries to deliver adequate O 2 to meet the needs of the myocardium.

E N D
Biology of Disease CH0576 Ischaemic Heart Disease (Coronary Artery Disease) CH0056/RHY
Ischaemic Heart Disease • A collective term to describe a range of conditions characterised by inability of the coronary arteries to deliver adequate O2 to meet the needs of the myocardium. • A number of factors govern the outcome of IHD: • The degree of coronary insufficiency • Rapidity of onset • Degree of collateral circulation CH0576/RHY
Ischaemic Heart Disease • The possible outcomes being:- • Chronic Ischaemic Heart Disease • Angina Pectoris • Myocardial Infarction • Sudden Death • IHD is by far the commonest form of heart disease in the industrialised world. • It is generally uncommon in the less developed areas of the world. CH0576/RHY
Aetiology & Risk Factors • A) Atherosclerosis: of the coronary arteries is by far the leading cause of IHD • Several risk factors have been identified for atherosclerosis, these are essentially the risk factors for IHD development. • The risk factors fall into two main groups: • Unmodifiable risk factors • Modifiable risk factors CH0576/RHY
Aetiology & Risk Factors • Unmodifiable risk factors: • Older age (patients are typically aged 35 – 65 years of age) • Male gender (after the age of 65, the rates of IHD are similar for both sexes) • A family history of premature IHD. CH0576/RHY
Aetiology & Risk Factors • Modifiable risk factors: • Hypertension • Cigarette smoking • Hypercholesterolaemia • Diabetes mellitus • Obesity • Physical inactivity • Psychosocial factors (e.g. stress) CH0576/RHY
Modifiable Risk Factors CH0576/RHY
Aetiology & Risk Factors • B) Other Causes: These include:- • Thromboemboli • Coronary Artery Spasm • Coronary Arteritis • Conditions which increase cardiac work load and oxygen demand: • Tachycardia, • hyperthyroidism, • catecholamine treatment. CH0576/RHY
Aetiology & Risk Factors • Conditions that decrease oxygen delivery to the heart:- • Anaemia • Hypotension • Carbon monoxide poisoning CH0576/RHY
Pathogenesis • Irrespective of the eventual clinical outcome, IHD almost always begins with athersclerotic changes in the coronary circulation. • A number of varying theories of the pathogenesis of atherosclerosis have been proposed. • A favoured theory is the ‘response to injury’ theory. CH0576/RHY
Response to Injury • This hypothesis accommodates all of the various risk factors which have been outlined for IHD. • Key features of the theory include: • The development of focal areas of endothelial injury. • Permeation of lipoproteins into the vessel wall • The lipoproteins are predominantly LDLs and VLDLs. CH0576/RHY
Response to Injury (key points) • A range of cellular interactions at the site of endothelial injury. • Cells involved in these interactions include • endothelial cells, • smooth muscle cells, • mononuclear phagocytes, • T-lymphocytes. • Proliferation of smooth muscle cells and the proliferation of elements of the extracellular matrix. CH0576/RHY
Response to Injury • Endothelial Injury: The injury to the endothelial layer in vivo is usually very subtle. Potential sources of injury include:- • Circulating endotoxins • Hypoxia • Products of cigarette smoke • Viruses • Specific endothelial toxins e.g homocysteine CH0576/RHY
Response to Injury • Probably of most importance as damaging events are: • Haemodynamic stresses • The effects of hypercholesterolaemia. • These two damaging events acting together will have a synergistic effect. • Turbulent flow increases endothelial permeability and cell turnover. CH0576/RHY
Response to Injury • Turbulent flow also increases receptor mediated LDL- endocytosis. • Leucocyte adhesion to endothelium is also increased. • The complex geometry of the arterial system gives rise to local turbulence. • This theory is supported by the increased incidence of plaque formation at specific sites:- CH0576/RHY
Response to Injury • The mouths of exiting vessels. • Branching points of arteries. • Along the posterior wall of the descending and abdominal aorta. • The concept of the ‘hammer and anvil’ • Hyperlipidaemia: The severity of any atherosclerosis has a direct correlation with serum levels of cholesterol or LDL. • Chronic hypercholesterolaemia may initiate endothelial damage itself. CH0576/RHY
Modified LDLs • Lipoproteins accumulate within the intima of vessel walls at sites of damage. • The lipid within the arterial wall is modified by oxidative mechanisms to yield modified LDLs. • Modified LDLs contribute to the pathogenesis by: • Being readily ingested by macrophages • Being chemotactic for monocytes • Increasing monocyte adhesion CH0576/RHY
Modified LDLs • They retain macrophages at the site of damage. • They stimulate the release of growth factors and cytokines. • They are cytotoxic to endothelial cells and smooth muscle cells. • They are immunogenic. • It may be possible to confer some protection against AS by the use of anti-oxidants such as Vit E. CH0576/RHY
Cellular Events • Cellular Interactions: • A complex range of cellular interactions, similar to those which occur in chronic inflammation, occur at the site of plaque formation. • Macrophages engulfing lipids become ‘foam cells’. • Smooth muscle cells migrate from the media into the intima and proliferate. CH0576/RHY
Cellular Interactions • In face of persistent hyperlipidaemia:- • Monocyte adhesion • Subendothelial migration of smooth muscle cells • Accumulation of lipids within macophages and smooth muscle cells, all continue. • Aggregates of these foam cells within the intima become obvious ‘fatty streaks’ • These can be evident in the vessels of individuals from an early age. • They are the forerunners of fully formed atheromas. CH0576/RHY
Cellular Interactions • With further persistent hyperlipidaemia the situation worsens. • Smooth muscle cells proliferate in response to cytokines. • There is collagen and extracellular matrix deposition. • Extracellular lipid accumulates. • The fatty streak is converted into a fibro-fatty atheroma – the atheromatous plaque CH0576/RHY
Cellular Interactions • The deposition of collagen and other extracellular matrix components produces a distinct ‘fibrous cap’ over the site. • As a consequence the vessel lumen becomes increasingly occluded ischaemia. • The endothelium above the atheroma is fragile and is prone to ulceration/damage. • Platelet aggregation and thrombosis are initiated at the sites of ulceration further ischemia. CH0576/RHY
Pathogenesis • Severe or fatal IHD often involves a >50% decrease in the diameter of at least one of the major coronary arteries. • Most severe narrowing is usually at:- • Proximal 2 cms of the left anterior descending and left circumflex coronary arteries (LAD & LCX). • Proximal and distal thirds of the right coronary artery (RCA) CH0576/RHY
Pathogenesis • Sudden thrombotic occlusion, due to ulceration or rupture of an atheromatous plaque seems to be the precipitating event of an acute myocardial infarct. CH0576/RHY
Commonest Sites of Coronary Artery Occlusion CH0576/RHY
Atheroma Stages in Aorta CH0576/RHY
Sites of MI & Vessel Involvement CH0576/RHY
Appearance of Myocardial Infarct (Early) Lateral MI Due to blockage of LCX artery Failure to perform oxidative reaction with NBT Light area is the infarcted site CH0576/RHY