Download
1 / 21
250 likes | 614 Views
Learn about the pathophysiology, clinical presentation, imaging features, diagnosis, and management of IgG-4 related autoimmune pancreatitis (AIP) and cholangitis, including histological characteristics, treatment options, and outcomes.

E N D
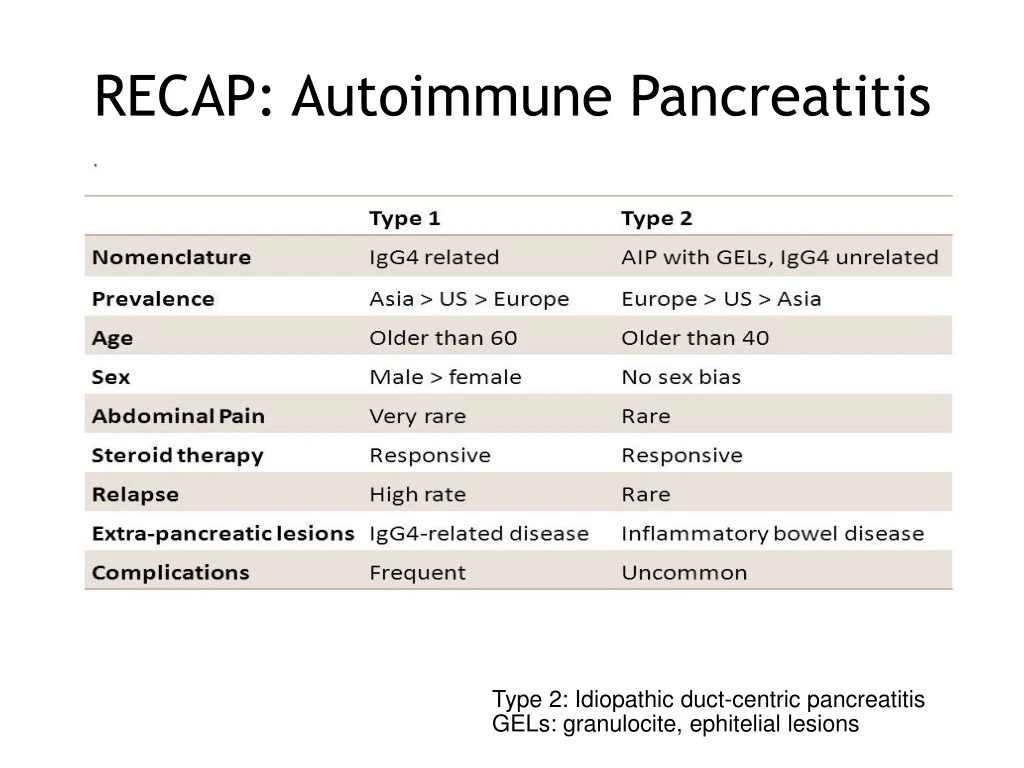
RECAP: Autoimmune Pancreatitis Type 2: Idiopathic duct-centric pancreatitis GELs: granulocite, ephitelial lesions
IgG-4 Related Diseases Various organ manifestations of a fibro-inflammatory condition characterized by tumefactive lesions recognised as a systemic condition in 2003 Linked by the same histopathological characteristics and elevated serum IgG4 concentrations. Multiple immune-mediated mechanism contribute to the fibro-inflammatory process, being autoimmunity and infectious agents potential triggers of a Th-2 and T-reg response.
Pathophysiology Stone J, Zen Y. IgG4-Related Disease N Engl J Med 2012;366:539-51.
IgG-4 Related Pancreato-biliary Diseases Majority of patients are men (60-73%), > 60 years Prevalence 0,2-0,8/100.000 Lack of familiarity! Up to 40% of patients have allergic diseases (atopy, eczema, asthma, chronic sinusitis) 30% normal serum IgG-4 concentrations IgG-4 related sclerosing cholangitis associated with AIP in 47–92% of pt
IgG-4 Pancreatitis Clinical presentation Acute vs Chronic symptoms Painless obstructive jaundice 33–60% Steatorrhea - exocrine functional abnormalities in up to 80% Abdominal pain 32% Back pain and weight loss 15% Serologic marker: titers of g-globulin (>2000 mg/dL) IgG (>1800 mg/dL) IgG4 (>140 mg/dL) Serum IgG4 >140 mg/dL 86% SN, 96% SP
IgG-4 Pancreatitis Imaging features Enlarged pancreas “sausage-like appareance” 50-70% Focal masses 30% Soft tissue hypoenhancing rim Narrowing of main pancreatic duct “Duct-penetrating” sign at secretin-MRCP
IgG-4 Pancreatitis Role of EUS-FNA Histological proof of the disease: GOLD STANDARD Exclusion of carcinoma Discrimination of type 1 from type 2 AIP Diffuse lymphoplasmacytic infiltration and storiform fibrosis IgG4-positive plasma cells > 10/hpf
IgG-4 Pancreatitis Hystology is the GOLD STANDARD: Diffuse lymphoplasmacytic infiltration with mild-moderate eosinophilia Obliterative flebitis and storiform fibrosis IgG4 immunostaining: > 50 IgG4 plasma cells/HPF for surgical specimens > 10 IgG4 plasma cells/HPF for biopsy samples RatioIgG4-positive/IgG-positive plasma cells > 40%
IgG-4 Pancreatitis: diagnosis The MAYO Clinic HISORt criteria
IgG-4 Cholangitis Clinical presentation 70% obstructive jaundice with pruritus and abdominal pain Asymptomatic jaundice less common than AIP 7-10% cirrhosis manifestation (hepatic failure, ascites, hepatic encephalopathy or variceal bleeding) Serologic marker: titers of g-globulin (>2000 mg/dL) IgG (>1800 mg/dL) IgG4 (>140 mg/dL) reumatoid factor, antinucleus antibody
IgG-4 Cholangitis Imaging features Isolated intrapancreatic CBD strictures Localized hilar hepatic lesion (strictures or masses) Intense and diffuse extension of bile duct wall homogeneousthickening (often circular) IDUS: inflamed submucosa and preserved epithelium, circular symmetric wall thickening
IgG-4 Cholangitis DD IDUS: eccentric wall thickening with an irregular luminal surface, disruption of the bile duct wall layered structure, and a hypoechoic mass with irregular margins
IgG-4 Cholangitis DD IDUS: all bile duct layers inflamed, bile duct epithelium severely damaged, disappearance of the three layers Imaging: diverticulum-like out-pouching, and beaded - tree appearance
Therapy INDUCTION 0,6-1 mg/kg oral prednisolone TAPERING 5 mg/wk reduction MAINTENANCE: 2,5-5 mg/die oral prednisolone or AZA Pancreatic enzyme supplementation (pancrelipasis) for exocrine insufficiency if: steatorrhoea, weight loss, metabolic bone disease, vitamin deficiency Oral hypoglicemic agents or insulin for diabetes mellitus Biliary stenting in obstructive jaundice (case-by-case)
Outcomes Spontaneous resolution in up to 30% Response to steroid therapy in 90% to 95% with improvement of imaging findings and serology within 2 weeks + symptoms regression New onset diabetes mellitus usually improves with corticosteroid therapy Chronic pancreatitis in about 10% Very rarely progression to cirrhosis in IgG-4 cholangitis
Outcomes Response to steroid therapy in 90% to 95% of both parenchymal and ductal changes Before (A) steroid therapy and after (B)
TAKE HOME MESSAGES • Suspect! • May have acute or chronic manifestation • Typical imaging findings (CT/MRI) • Mandatory is exclusion of carcinoma • Characteristic histopathological appearance: histology is the GOLD STANDARD • Not always elevated IgG and IgG-4 levels • Systemic disease: look for biliary and retroperitoneal involvement
Bibliografia • Stone J, Zen Y. IgG4-Related Disease N Engl J Med 2012; 366: 539-51. • Kamisawa T, Zen Y. Advances in IgG4-related pancreatobiliary diseases. Lancet Gastroenterol Hepatol 2018; 3: 575–85. • Sandrasegaran K, Menias C. Imaging in Autoimmune Pancreatitis and Immunoglobulin G4–Related Disease of the Abdomen. Gastroenterol Clin N Am. 2018. Article in press.