Interventional Radiology
Interventional Radiology. North Shore Medical Center. The “Ins and Outs”. Needles Catheters Guide Wires Tubes Ya-Da-Ya-Da-Ya-Da!!!!. Introduction.


Interventional Radiology
E N D
Presentation Transcript
Interventional Radiology North Shore Medical Center
The “Ins and Outs” • Needles • Catheters • Guide Wires • Tubes • Ya-Da-Ya-Da-Ya-Da!!!!
Introduction • Purpose: to discuss a brief history of Interventional Radiology, the current interventional procedures done at the NSMC, the radiology nurse’s role and the impact on patient care in the Radiology Department • To educate floor and recovery room nurses about the pre and post care of the IR patient • Joyce Silvano, RN, ANM Radiology
Topics of Discussion • Definitions and Brief History • Vascular and Non-Vascular Interventional Radiologic Procedures • Pre, Intra, and Post Procedure Nursing Care • Follow-up Care
Definitions • INTERVENTIONAL RADIOLOGY (IR) • minimally invasive procedures and targeted treatments using image guidance • small instruments guided through the blood vessels or other pathways to treat diseases percutaneously
Definitions • INTERVENTIONAL RADIOLOGIST • medical doctors who specialize and are board certified in performing procedures using medical imaging • assume responsibility for the patient’s care before, during, and after the procedure • INTERVENTIONAL RADIOLOGY NURSE • critical care RN who provides continuous quality care for the patient requiring an interventional procedure
Interventional Radiology Nurse • Patient advocate • Patient educator • Responds to medical emergencies within the entire department 1. Contrast Reactions 2. Seizures 3. Vasovagal Reactions 4. Cardiopulmonary Arrest • Liaisons – communication between radiology and patient care floors, referring facilities, or doctor’s offices • Long-term Goal: continue to provide educational opportunities to our fellow nurse’s
Brief History • 1967, Dr. Alexander Margulis coined the phrase “interventional diagnostic radiology” • Mid 70’s: Improved radiologic imaging and development of tools Balloon Catheters Wires • Interventional Radiologists pioneered coronary angiography, invented angioplasty and catheter-delivered stents
Brief History • 1992: AMA officially recognized IR as a medical specialty • 2001: Society of Interventional Radiology (SIR) adopted the following definition: “Interventional radiology is the medical specialty devoted to advancing patient care through the innovative integration of clinical and imaging-based diagnosis and minimally invasive therapy.”
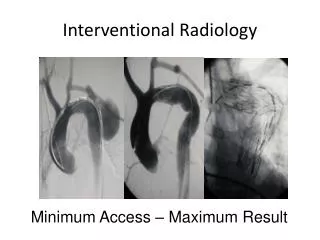
Vascular Interventions • Angiography/Angioplasty/Stents • venous and arterial • Fibrinolytic Therapies • venous and arterial • Embolization Therapies • IVC Filter Insertions (mostly retrievable) • Venous Access Device Insertions • Implanted VAD • Dialysis Catheters: Temporary and Permanent • PICC and CVC insertions
Non-Vascular Interventions • Biliary Interventions • Percutaneous Cholangiograpy and Biliary Drainage Catheter Insertion • Cholecystostomy • Biliary Stone Removal • Biliary Strictures: Dilitations and Stent Insertions • GI Interventions • Percutaneous Gastrostomy/Gastrojejunostomy • GI Strictures: Dilitations and Stent Insertions • GU Interventions • Antegrade Pyelogram/Nephrostomy • Nephroureteral and Ureteral Stent • Renal Stone Manipulation
Non-Vascular Interventions Cat Scan and Ultrasound • Biopsy and/or Fluid Aspirations • Thoracic (lung, pleural, and mediastinal) • Retroperitoneal Lymph Nodes • Hepatobiliary ( liver: focal abnormality/targeted or for liver medical disease, increased LFT’s or Hep C) • Pancreas • Spleen • GU (renal: focal abnormality/targeted; medical renal disease; bladder, urethra, prostate) • Soft Tissue (superficial or deep) • GI Mesenteric • Adrenal • Peritoneal • Muskuloskeletal (bone, joint, muscle) • Neuro-spinal • Thyroid
Drainages Abscess/Infections • Thorax – empyma • Retroperitoneal • Intraperitoneal • Visceral/Organ • Superficial Non-Infected • Pleural (effusion, pneumothorax) • Mediastinal • Retroperitoneal • Intraperitoneal (ascites) • Visceral/Organ (cyst aspiration) • Superficial
Drainages (continued) Sclerosis • Thoracic • Retroperitoneal • Intraperitoneal • Visceral • Pain Management • Neuro-blockade • Vertebroplasty
Pre-Interventional Procedures • Labs: BUN, Creat, eGFR, E-Lytes; Coags, CBC, FSBS on arrival if not done at home; urine HcG; fibrinogen and type and screen for fibrinolytic therapy; type and screen for RFA and medical renal biopsy; EKG for all PVD patients and patients receiving anesthesia • Consent/History & Physical • Nursing Assessment with Medication Reconciliation • Procedural Teaching • Pre-procedure instructions for outpatient (telephone screening if no consult) • Renal agram patients: Hold long acting antihypertensives if renal angioplasty is likely • eGFR < 60: Mucomyst 600mg twice a day 24 hours prior and on the day of the contrast and/or Bicarb drip 3 ml/kg for 1 hour prior to contrast exposure and 1 ml/kg during exposure and for 6 hours post contrast • Prior contrast reaction: Pre-medicate with prednisone and diphenhydramine • Anticoagulants: Coumadin, Heparin, Lovenox, Fragmin • Antiplatelet therapy: ASA products, Vitamin E, the 3 G’s, Fish Oil, Plavix • Site marking and patient identification outside of the procedure room
Intra-procedure care • Procedural Sedation when indicated • Circulator for anesthesia cases • Monitor patient continuously during procedure • Report any abnormal changes in vital signs or patient condition to the interventional radiologist • Reassure patient, explain what will happen next • Reassess patient frequently for pain, change in condition and intervene as appropriate
General post-procedure care • Post-procedure instructions: patient, family member if procedural sedation used • Maintain IV access until discharged • Monitor puncture site, wound, etc. until patient transferred to nursing unit or discharged home • Reassess condition, vital signs, pain as above • Document assessments and discharge criteria on flow sheet • Handoff report to accepting floor or outside facility • Discharge instructions given to and reviewed with patient and family member (may be done prior to procedure by IR RN)
Diagnostic Imaging Procedures • Lumbar Puncture • 2 hour recovery • Flat x1 hour • Pre procedure - No dietary restrictions; Post procedure - encourage caffeinated fluids if no contraindication • Outpatients may drive home • Myelogram • 2 hour recovery • Flat x 1 hour • Pre procedure - light breakfast then clear liquids; Post procedure – same as lumbar puncture • Patient requires ride home • Discharge instructions to include time frame and symptoms of post puncture headache (slow leak may take up to 3-5 days to exhibit symptoms nausea and vomiting; unable to lift head off of pillow) • Arthrogram
Next Steps Peripheral Vascular Angioplasty/Stents
Post-UAE Pre-UAE
Other Indications for Embolizations • Arterial bleeding d/t tumor erosion • Epistaxis • AVM/Cerebral Aneurysms • Uncontrollable post-partum bleeding • Inadvertent arterial injury during surgery
General Post Angiography Care • Arterial puncture site • Femoral stick: lower extremity extended and still x 2-4 hours with closure device; x 6-8 hours manual compression, may log roll side to side • Axillary stick: keep arm in sling and still for 6-8 hours and assess for brachial plexus injury • HOB 30 degrees • Monitor puncture site(s) for hematoma • Apply direct pressure to puncture site and call IR • Retrograde stick – Index finger on and two fingers above puncture site • Antegrade stick – Index finger on and two fingers below puncture site • CONFUSED? Middle finger on the puncture site with one finger above and one below • Monitor vascular status of the extremity distal to puncture site to include pulse checks, csm and temperature assessments • Venous puncture site • Extremity still for 2-4 hours • Monitor for signs of bleeding • Encourage oral fluid intake for those patients able to drink to help excrete contrast and prevent nephrotoxicity • DO NOT ADMINISTER PROTAMINE SULFATE FOR REVERSAL OF HEPARIN TO ANY PATIENT THAT HAS RECEIVED NPH (neutral protamine Hagedorn) INSULIN. This may percipitate an anaphylactic reaction… • Give smoking cessation information to any patient with peripheral vascular disease that continues to smoke • Encourage patient to exercise regularly • Discharge Instructions: NSMC Clinical Med Rec Froms
Specific Angiographic Potential Post Procedure Complications • Renal angioplasty +/- stent insertion • Hypotension especially if patient takes multiple antihypertensive medications and long acting drugs have not been discontinued • Worsening renal function or failure with peripheral renal emboli (not immediately evident) • Embolization procedures • Ischemic pain distal to embolization: UAE, iliac artery (pre endo graft repair of AAA) • Misembolization
Indications, Goals, Complications • Combined IR/OR procedure in OR suite • Emergent or Elective • Known or suspected rupture or rapidly expanding rupture • Less invasive alternative for low risk patient decreasing procedural morbidity & mortality; post procedural pain and complications; decrease in hospital stay (2 days low risk patient and 4 days high risk patient) • Provides treatment to high-risk patients who are not surgical candidates and would have no other therapeutic options • Major Complications • MI, CHF, Hypertension, DVT, Stroke, GI and RP hemorrhage, HIT, limb ischemia +/- amputation, pseudoaneurysm, renal failure, infection, surgical conversion
Venous Access Devices • PICC/CVC • Implanted VAD • Dialysis Catheters/Temporary and Permanent • Hickman Pheresis Catheters
Post Biopsy Care • Lung Biopsy • Usually FNA’s (Fine Needle Aspirations) only • CXR 1 hour and 3 hours post biopsy • Immediate CXR for chest pain, dyspnea, decreasing sats • Biopsy side down x 3 hours (may sit up to eat after 1 hour CXR) • NPO until 1 hour CXR read and is okay • Blood tinged sputum is to be expected, large amount of hemoptysis contact IR MD • Pneumothorax: Continue supplemental O2 • May transfer to recovery with small, stable ptx • PTX may be aspirated prior to transfer • Abdominal/Organ biopsy • Biopsy site down x 3 hours (liver/renal) • Liver biopsy – always core sampling for non targeted biopsy • Stretching of the liver capsule may cause moderate to severe pain • Pain may radiate to the shoulder • Advance diet as tolerated • All Biopsy patients • Up to 4 hour recovery time • Assess for signs of hemorrhage or infection – Non targeted renal biopsies (core) stay 23 hours to monitor HCT’s • Discharge Instructions NSMC Clinical Med Rec Froms
Percutaneous Nephrostomy PCN – External drainage of the renal collecting system • Ureteral obstruction causing a hydro or pyonephrosis; tumor, pregnancy, stone. • Tract creation for lithotripsy with guide wires left in place • Urinary diversion to allow healing of ureteral leaks or fistulas • May be short term; tract for lithotripsy, decompression from infection, pre and post stent insertion (safety catheter) • May be long term; maintain drainage in patients with malignant tumors compressing the collecting system, uni or bilateral.
Post PCN Care • Observation for up to 4 hours • Monitor for signs of retroperitoneal bleeding • Vital sign changes • Severe flank pain • Drop in HCT without hematuria • Monitor for hematuria • Blood tinged urine output expected for the first 48 hours • Gross hematuria – call MD • Forward flush catheter with 10 ml NS • Maintain catheter patency - no kinks • Observe for drainage around catheter at skin site • Decreased urine out put • Bladder Spasms • Discharge Instructions NSMC Clinical Med Rec Forms
Post Vertebral Augmentation Care • Flat for 2 to 4 hours • Advance diet as tolerated • Watch for signs of complications • Chest pain/hypoxemia – pulmonary cement embolus • Neurological changes – CNS cement embolism • Loss of bowel or bladder control • Lower extremity weakness • Fractured Rib • Temporary worsening of pain may occur
TIPS –Transjugular Intrahepatic Portosystemic Shunt • Reroutes blood flow to reduce complications from portal hypertension and varices • Reduces portal vein pressure by creating a decompression channel between a hepatic vein and an intrahepatic branch of the portal vein • Usually done emergently because of hemorrhage from varices • May be performed electively for refractory ascites • Stent placed from portal vein directly through liver to hepatic vein • Lasts 1-4 hours • Usually done under general anesthesia Potential Complications • Encephalopathy: toxic substances in the bloodstream are ordinarily filtered out by the liver. The TIPS may cause too much of these substances to bypass the liver filtration, so a patient who already has encephalopathy because of their liver disease may not be a good candidate for the procedure. • bleeding into and around liver • occlusion or stenosis of stent • pulmonary edema from elevated cardiac output, cardiac index and RA pressures (especially in acutely bleeding patient receiving fluid resuscitation)
Radiofrequency Ablation (RFA) • Minimally invasive procedure under CT or US guidance • Special needle electrode placed in a tumor • Most often primary liver or colon met to liver, can be done for renal, lung and bone lesions • Effective treatment in patients unsuitable for surgery, failed chemotherapy, recurrence after surgery, multiple lesions • Treated in one or more sessions, minimal discomfort, outpatient procedure • Radiofrequency current passed from generator through the electrode to heat the tumor tissue near the needle tip destroying cancer cells and a small rim of normal liver tissue • Closes small blood vessels, minimizing risk of bleeding
Radiofrequency Ablation (RFA) • Risks of liver RFA include brief shoulder pain, inflammation of gallbladder, damage to bile ducts with resulting biliary obstruction, thermal damage to bowel or adjacent structures • “Post-ablation syndrome” flu-like symptoms that appear 3-5 days post procedure, lasting about 5 days, treated with acetaminophen