Download
1 / 1
10 likes | 167 Views
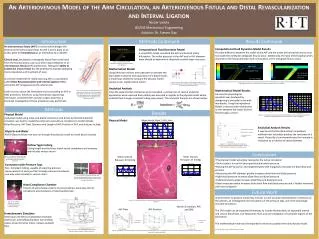
An Arteriovenous Model of the Arm Circulation, an Arteriovenous Fistula and Distal Revascularization and Interval Ligation. Vena Cava. Aorta. Subclavian. Axillary. Nicole Varble BS/MS Mechanical Engineering Advisor: Dr. Steven Day. PROX Vein. PROX Brachial. AVF. DIST Brachial.

E N D
An Arteriovenous Model of the Arm Circulation, an Arteriovenous Fistula and Distal Revascularization and Interval Ligation Vena Cava Aorta Subclavian Axillary Nicole Varble BS/MS Mechanical Engineering Advisor: Dr. Steven Day PROX Vein PROX Brachial AVF DIST Brachial Introduction Objectives Introduction Methods Continued Results Continued Collateral DIST Vein An arteriovenous fistula (AVF) is a vessel which bridges the arterial to the venous blood flow. An AVF is put in place as an access point for hemodialysis as an alternative to a catheter. Clinical steal, decreased or retrograde blood flow to the hand from the brachial artery, can occur after implementation of an arteriovenous fistula (AVF) anastomosis. Having the ability to predict the onset of steal has the potential to improve operating room procedures and treatment of steal. A common treatment for malfunctioning AVFs is a procedure called Distal Revascularization and Interval Ligation (DRIL), where the AVF is bypassed on the arterial side. Little is known about the hemodynamics surrounding an AVF or DRIL procedure, therefore, using mechanical engineering techniques, combined with vascular surgery expertise, a thorough investigation of these procedures was performed. Ulnar Computational Fluid Dynamics Model Results Pressure difference between the outlet of the AVF and the outlet of the brachial artery must not exceed 10 mmHg for antegrade flow to occur. Additionally, the ratio of the brachial artery diameter to the fistula diameter must not exceed 1.25 for antegrade flow to occur. Computational Fluid Dynamics Model A simpleCFDmodel simulated the AVF and brachial artery bifurcation. The outlet pressure of the AVF and to AVF diameter were altered to determine a threshold at which steal may occur. Radial Hand Compliance Figure 6- The brachial artery/AVF bifurcation modeled and meshed in ANSYS, a CFD software Mathematical Model Using electrical resistors and capacitors to simulate the equivalent resistance and capacitance of a blood vessel, a model was created to compare the physical model results to this mathematical model 1.43e+00 Figure 10- A velocity vector plot of retrograde flow occurring when the difference between the AVF and brachial artery outlet pressure is 20 mmHg (left), and a velocity magnitude plot of the an enlarged AVF where maximum velocity is shown in red (right). 8.73e-03 Figure 7- The sin wave driving the mathematical model with two damping diodes (left). The brachial artery modeled in Simulink using two resistors and a capacitor. (right). Analytical Analysis Once the experimental resistances were calculated, a comparison of several analytical approaches were used and their validity was assessed in regards to the physical model where pulsatile flow through compliant tubing was present. The analytical theories are shown below: Mathematical Model Results An accurate physiological waveform was produced by dampening a sinusoidal curve with two diodes. Using the Impedance Model, a second order relationship is seen between the radius and the flow through a vessel. Figure 1- The AVF (white) moves blood from the arterial to the venous side. The arterial bypass (DRIL) passes over the AVF and is revascularized at a distal location of the arterial blood flow. The arterial ligature (interval ligation) is just distal to the AVF [1]. Methods AVF Results Physical Model A physical model using tubes and plastic connectors and driven by the hemodynamic simulator, was built to model the entire arm vasculature. Variations to model include: Blood Pressure, AVF Flow, Diameter and Length of AVF, Position of AVF, and features include: Figure 11- The pulsatile waveform generated in Simulink (left), and the relationship between AVF diameter and distal (hand) flow when the Impedance model is used (right). Retrograde Flow Physical Model Mean Aortic Flow: 5.45 L/min dP = 20 mmHg Analytical Analysis Results It was found that the Womersley’s Impedance method most accurately predicts the resistance of a vessel. Poiseuille’s Law overestimates the increase in resistance as a function of vessel diameter. • Glycerin and Water • 40/60 Glycerin/Water mix was run through the physical model to match blood viscosity Figure 12- The experimentally found resistances as compared to the analytical impedance method is shown to closely predict the resistances in a pulsatile vessel. Hollow Tygon tubing Tubing length and thickness match vessel compliance and anatomy and includes venous return Brachial Artery Conclusions Mean Venous Pressure: 27 mmHg Mean Arterial Pressure: 92 mmHg Figure 2- The subclavian artery made with clear Tygon tubing and equipped with the ME PXL10 flow probe and pressure transducer. • The physical model accurately represents the native circulation • Clinical steal is a result of decreased brachial artery pressure • Moving the AVF proximal and lengthening the AVF marginally increases the distal flow and pressure • Decreasing the AVF diameter greatly increases distal flow and distal pressure • High blood pressure increases distal flow and distal pressure • Collateral blood supply increases distal flow and distal pressure • Distal revascularization increases both distal flow and distal pressure and is further improved with interval ligation Connectors with Pressure Taps Non- Compliant tubing, capable of acquiring pressure measurements at each junction through pressure transducers, one-way valve included in venous return 1.17e+00 Figure 3- The brachial- collateral bifurcation, adapted with a pressure tap (left). The brachial- AVF bifurcation adapted with a pressure tap and shown with the leur lock assembly (right) to easily connect to pressure transducers. DRIL 0.00e+00 Hand Compliance Chamber Column of water below column of pressurized air, accurately mimics compliance and resistance of hand capillary bed Future Work df = 6.16 mm db = 4.4 mm ratio: 0.7 Improvements to physical model may include, a more accurate representation of stenosis of the arteries, an investigation into the patency of the pressure taps, and more physiologic accurate connectors. The CFD model can be expanded immensely to include flexible walls, an expanded arterial and venous blood flow, non-Newtonian fluid, and an investigation of turbulent regions of the bifurcation. The mathematical model can be expanded to more accurately mimic the physical model. Figure 8- The complete artierovenous physical model capable of producing physiologic pressure and flow waveforms. Figure 4- The unfilled compliance chamber after the radial and ulnar arteries converge. Native Circulation, AVF, and DRIL AVF Flow AVF Position Hemodynamic Simulator Ventricular and Venous Compliance chamber, ventricular and buffing chamber, two artificial valves, driven by Servo motor, outputs pulsatile flow [1] "ACS Surgery," Decker Intellectual Properties, 2010. Figure 5- Schematic of RIT MSD P09026 Hemodynamic Simulator (image created to Matthew DeCapua) Figure 9- The effects on the distal (hand) flow and pressure when the flow through the AVF is altered (left), when the position is altered (center), and when the DRIL bypass procedure is implemented (right).