Download
1 / 23
230 likes | 402 Views
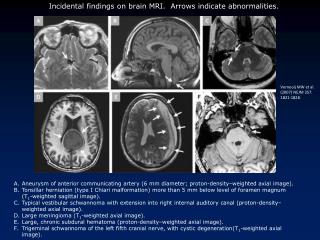
Single-Dose Perinatal Nevirapine plus Standard Zidovudine to Prevent Mother to Child Transmission of HIV-1 in Thailand. NEJM July 15, 2004 Lallemant et al. UNAIDS & WHO Update Dec 2004. Geographical Distribution of People Living with HIV/AIDS.

E N D
Single-Dose Perinatal Nevirapine plus Standard Zidovudine to Prevent Mother to Child Transmission of HIV-1 in Thailand NEJM July 15, 2004 Lallemant et al.
Factors determining Maternal to Child Transmission of HIV-1 • High maternal viral load • Low maternal CD4 cell count • Illicit drug use • Birth weight < 2500 grams • Rupture of membranes > 4 hours • Virulence factors of HIV strain • Host susceptibility factors
Mother to Child Transmission of HIV-1 • In utero • Perinatally • Breastfeeding
The “When” of MTCT of HIV-1 • Risk of transmission in those receiving no antiretroviral therapy ~25% overall * Moment of Birth (Perinatal): 70% Antenatal Period : 30%
Some History: PACTG 076 TRIAL • Multi-centered, double blind, placebo controlled • Women with HIV (not AIDS) • CD4 count > 200 • No clinical symptoms of AIDS • ZDV during 2nd and 3rd trimesters • IV ZDV during labor & delivery • ZDV to infant 0 - 6 weeks Connor EM et al N Engl J Med 1994, 331:1173-80.
Results of PACTG 076 trial • Mother - Infant dyads: • 23% transmission in controls • 8% transmission in treated • Overall 67.5% relative reduction in risk of HIV transmission during labor!
This is HUGE! • Why? • The study that showed that transmission ofHIV could be prevented by antiretroviral therapy… Applies to: • MTCT • Needlestick accidents
The “Thai Regimen” • 1999, MPH provides short course AZT to HIV-infected women in 3rd trimester • Transmission rates >6% STUDY IDEA: • Add single dose nevirapine (sdNVP) perinatally to lower transmission rates *hypothesis: the addition of sdNVP to a 3rd trimester regimen of AZT is superior to short-course AZT alone for preventing MCTC of HIV-1
Study design • Multicenter • Phase 3 (safety and efficacy evaluation) • Double-blind • Randomized • Placebo-controlled
Inclusion criteria AZT received at 28 weeks gestation or asap after (at least for 2 weeks) “health” screen before randomization Written consent Agreement not to breastfeed Exclusion criteria - maternal/fetal condition or treatment that contraindicated treatment with NVP or AZT Patients
Experimental Treatments • Patients were randomized to 3 groups: • NVP-NVP (NVP dose to mom and baby) • NVP-placebo (NVP to mom, placebo to baby) • Placebo-placebo (placebo to both) *Study powered to evaluate the superiority of the NVP-NVP arm over the placebo-placebo arm
Evaluation • Follow-up: • mother: every 2 weeks predelivery, postdelivery at 10 days, 6 weeks, 4 months • Infant: 10 days, 6 weeks, 4,6,8,12 months • Evaluation of infant for HIV-infection: • Peripheral blood/Amplicor Assay • + if 2 positive PCR on 2 different occasions • - if 2 negative PCR on 2 different occasions after age of 1 month
Results – Part 1 First interim (40% women enrolled) - NVP-NVP: 1.1% transmission - NVP-placebo: 2.1% transmission - placebo-placebo: 6.3% transmission *Placebo-placebo group discontinued; study restructured to show noninferiority of NVP-placebo to NVP-NVP
Results – Part 2 • Final analysis - NVP-placebo: 2.8 % transmission - NVP-NVP: 1.9% transmission * difference not statistically significant
Discussion • NVP-placebo noninferior to NVP-NVP for lowering risk of transmission Problems: • True transmission rates: stratification by viral load (NVP-placebo had lower median viral load) and T cell counts • Ethical concerns: exposing mothers to NVP
More about Ethics • The problem with NVP: - long t1/2 - levels detectable 21 days later - single mutation confers resistance to NNRTI class of antiretrovirals • Women from the same study – those exposed to NVP had higher rates of virologic failure at 6 months of treatment with an NVP-containing regimen than those that were not exposed to NVP Jourdain G et al N Engl J Med 2004, 351: 229-238.
What about breastfeeding? • Meta-analysis estimates 14-24% transmission • Critical for parts of the world where safe alternatives not available • Recommendations: • 1985 CDC: against breastfeeding • 1987-92 WHO: regions where infections and malnutrition profound – continue breastfeeding • 1996 UNAIDS- allow mothers to make informed choice
Thanks to: • Dr. Marian Michaels • Krista Pfaendler • Dr. John Mellors

![Koepke et al., [1997] Kaufman and Tanre [1997] Levy et al., [2004] Remer et al., [2006]](https://cdn2.slideserve.com/3945504/slide1-dt.jpg)