Download
1 / 28
290 likes | 494 Views
Total Ankle Arthroplasty: A Unique Design 2-12 year follow-up. By Frank Alvine, M.D. et al University of Iowa Presented by Adam Morse, D.O. Garden City Hospital. Introduction. The results of TAA have not been comparable with those of other major joints

E N D
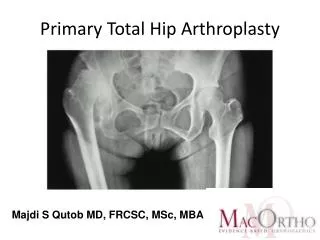
Total Ankle Arthroplasty: A Unique Design 2-12 year follow-up By Frank Alvine, M.D. et al University of Iowa Presented by Adam Morse, D.O. Garden City Hospital
Introduction • The results of TAA have not been comparable with those of other major joints • In 1982, Newton concluded that the results of TAA in patients with RA are so poor, that the procedure should be contraindicated • Bolton-Maggs agreed with Newton and further concluded that arthrodesis should be considered the treatment of choice for a painful stiff ankle reguardless of the underlying pathologic process
Introduction • The olny options available for debilitating end-stage DJD of the ankle are arthrodesis and arthroplasty • Problems with arthrodesis include: difficulty in achieving an adequate position of fusion, pseudarthrosis rates of 40-50%, infection rates from 0-22%,amputation rates as high as 13%, and persistent pain or limp • Patients with arthrodesis have difficulty climbing stairs, walking on uneven surfaces, and running
Introduction • Good clinical results with arthrodesis range from 65-100% • Waters reported that after successful TAA patients had a 16% decrease in gait velocity, 3% increase in O2 consumption, and a gait efficiency of 90%. • The smaller mid and forefoot joints didn’t experience the level of increased demands seen with arthrodesis
Introduction • According to Bauer et al, the long term results of constrained and unconstrained designs have been disappointing • High rates of loosening are seen with the constrained designs • Non-constrained designs have problems with instability and impingement
Materials and Methods • Agility ankle prosthesis (Depuy, Warsaw, Indiana), semiconstrained with a titanium tibial component and cobalt chromium talar component, tibial polyethylene component is 3.73-4.7mm thick depending on size • Permits flexion-extension arc of 60 degrees • Available in small, medium, and large • requires arthrodesis of distal tib/fib syndesmosis
Materials and Methods • The talar component is slightly wider anteriorly which theoretically makes it more stable in dorsiflexion • Tibial and talar components were both titanium initially, until 2 talar components loosened within three years • Tibial component was made thicker because of breakage of 2 components
Operative Technique • Supine, tourniquet, sand bag under hip • EBI Ex-fix placed for alignment and distraction • Anterior approach to the ankle between tibialis anterior and EHL tendons • Anterolateral approach to syndesmosis, AITF ligament elevated, cartilage denuded, bone grafted and 2 compression screws placed across the syndesmosis once prosthesis is in place
Operative Technique • 5-6 mm of bone is removed from the talus and distal tibia/fibula articular sides with the cutting jig • uncemented sized prostheses are then placed • Fixator is removed, skin is closed, posterior splint is applied and worn 23 hours/ day for 6weeks while NWB • Patient removes the splint TID for ROM exercises
Patient Demographics • 100 consecutive TAAs were evaluated • 1984-1993 with 2.8-12.3 year f/u (ave 4.8) • 5 Bilateral, 95 patients, 50 M and 45 F • Preoperative Diagnosis was RA-22%, PTOA-52%, Primary osteoarthrosis-22%, Septic arthritis-2%, and Psoriatic arthritis-1% • No workers Comp, 1 case under litigation for MVA
Patient Demographics • Average age 63 years (range 27-81) • 12 patients 14 ankles died prior to latest f/u • 1 required removal of components and fusion of the ankle • 85 ankles were left for evaluation • X-rays were taken pre-op, early post-op, at 6 months, 2 years, and at most recent follow up
Clinical Evaluation • Carried out by 2 independent physicians who did not perform the surgery • Interview, clinical examination, and x-rays were performed on 56 ankles, 54 patients • Remaining 29 ankles, 28 patients completed detailed written and telephone surveys, and sent films done locally • Questions related to level of pain, function and satisfaction with the procedure
Clinical Evaluation • PE included N/V status, alignment while standing, and ROM • An American Orthopedic Foot and Ankle Society hindfoot score was then calculated based on a 100 point scale
Radiographic Evaluation • NWB AP, Lateral, and Mortise views • Multiple line and angles were measured • Migration was defined as a minimum of 5 degree shift in the measured angle based on reliability and and rotational effect of radiographic positioning • Lucency was defined by radiolucent line <2mm thick around the prosthesis
Radiographic Evaluation • Ballooning lysis was an area greater than 2mm of lucency • The x-rays were divided into lucency zones 3 on the lateral, and 6 on the AP and Mortise • Fusion of the syndesmosis was described as Union, delayed union if >6 mo, and nonunion
Radiographic Evaluation • The lateral radiographs were used to determine the progression of other joint arthritis in the foot in the talonavicular, calcaneocuboid, and subtalar joints
Complications • One TAA was converted to an arthrodesis at 2 1/2 years in a patient with RA • 4 patients required revision • 2 tibial components fractured (only 1 wanted a revision, as the other was asymptomatic • No deep infections, 2 superficial infection treated with PO antibiotics • 6 patients lost sensation in the superficial peroneal nerve dermatome without functional problem
Clinical Results • 55% reported no pain • 28% reported mild pain • 16% reported moderate pain • None reported severe pain • 98% stated pain improved after surgery • 79% were extremely satisfied with the result • 13% were satisfied • 4% were indifferent • 4% were disappointed / very unhappy
Clinical Results • 95% would have the operation again • 96% would recommend the operation to a friend • 73% reported an increase in their functional level • 83% were taking no pain medicine for the ankle including all of the bilateral ankles • Only 40% of posttraumatic arthritis ankle were pain free • Both patients with septic arthritis had moderate pain
Clinical Results • No association was found between age and weight of the patient and postoperative pain • 68% reported they felt more comfortable walking in shoes with small heels • 4 patients used a cane, 3 wore a brace for valgus deformity • Of the patients with deformity 2/3 had moderate pain • Average sagittal plane ROM was 36 degrees
Clinical Results • 50% had a plantar flexion contracture • Contractures averaged 7 degrees • 11% dorsiflexed to neutral • 39% dorsiflexed beyond neutral averaged 4.6 degrees • 45% were not able to climb stairs as well as they would like to….. • Only 27% blamed the ankle for this • AOFAS hindfoot score averaged 85 points
X-Ray Results • 62% had a successful fusion of the syndesmosis • 29% had a delayed union • 9% had a non-union • 19 components (7 talar, 12 tibial) had 5 degrees of change on x-ray indicating probable migration • 8 of 12 tibial migration were associated with delayed or non-union
X-Ray Results • 55% of nonunions had tibial migration, 11% of delayed unions, and 7% of unions • Nonunion was also clearly associated with ballooning lysis in all cases, in 64% of delayed union, and 28% of solid union • Tibial components placed in more that 4 degrees of valgus had a significantly higher rate of pain
X-Ray Results • No appreciable progression of degenerative changes was observed in the talonavicular, calcaneocuboid, or subtalar joints • no relationship between age, weight, or preoperative diagnosis and the development of lysis, lucency, or migration of the component
Discussion • Radiographic lucency rates were very concerning • Non or delayed union of the syndesmosis was associated with a much higher rate of ballooning lysis • Lucent lines were always apparent by 2 years and were not progressive, including those with ballooning lysis with was thought to represent a lack of fixation
Discussion • 5 revisions were performed in the 100 patients by an average of <5 years • Implants placed without cement seem to be fairing better than those placed with cement
Presenter’s Conclusions • TAA is a long way from being a comperable alternative to arthrodesis • Significantly longer follow up will allow a better understanding of both the true longevity of the prosthesis, and well as the results of revision surgery, and conversion surgery to arthrodesis • At this point I believe that TAA should be referred to a large center where studies are ongoing, and only if patients refuse an arthrodesis

![Our top 10 B2B email marketing campaigns [and why they work]](https://cdn4.slideserve.com/7375820/slide1-dt.jpg)
