Download
1 / 49
700 likes | 2.23k Views
Cerebellum and Basal Ganglia in Motor Control. http://www.pennhealth.com/encyclopedia/em_DisplayAnimation.aspx?gcid=000016&ptid=17. The cerebellum and its motor functions. Based on cerebral intent and external conditions.

E N D
Cerebellum and Basal Ganglia in Motor Control http://www.pennhealth.com/encyclopedia/em_DisplayAnimation.aspx?gcid=000016&ptid=17
Based on cerebral intent and external conditions The cerebellum tracks and modifies millisecond-to-millisecond muscle contractions, to produce smooth, reproduciblemovements
Cerebellum and Its Motor Functions • It helps to sequence motor activities • And makes adjustments in the body’s motor activities while they are being executed so that they will conform to the motor signals directed by the cerebral motor cortex and other parts of the brain • The cerebellum also aids the cerebral cortex in planning the next sequential movement
Cerebellum and Its Motor Functions • The intermediate zone is concerned with controlling muscle contractions in the distal portions of the upper and lower limbs • The lateral zone is involved in overall planning of sequential motor movements
Topographical Representation of the Body in the Vermis and Intermediate Zones • Axial portions of the body lie in the vermis • Limbs and facial regions lie in the intermediate zones
Neuronal Circuit of the Cerebellum • Input Pathways to the Cerebellum: • Afferent pathways from the other parts of the brain: • Corticopontocerebellar pathway: originates in the cerebral motor and premotor areas and also in the somatosensory cortex • It passes pontile nuclei and pontocerebellar tracts mainly to the lateral divisions of the cerebellar hemispheres • Olivocerebellar tract: is excited by fibers from the motor cortex, basal ganglia, reticular formation and spinal cord • Vestibulocerebellar fibers: • Reticulocerebellar fibers:
Neuronal Circuit of the Cerebellum • Afferent pathways from the periphery: • Dorsal spinocerebellar tract: comes mainly from the muscle spindles, and to a lesser extent from other somatic receptors such as Golgi tendon organs • Muscle contraction • Degree of muscle tension • Positions and rates of movement of the body parts • Forces acting on the surfaces of the body • Ventral spinocerebellar tract: is excited mainly by motor signals arriving in the anterior horns of the spinal cord (efference copy of the anterior horn motor drive)
Output Signals from the Cerebellum • Deep cerebellar nuclei and the efferent pathways • Dentate • Interposed • Fastigial nuclei • All these deep cerebellar nuclei receive signals from • The cerebellar cortex • Deep sensory afferent tracts to the cerebellum • Excitatory signals to the deep nuclei and corresponding cerebellar cortex areas • Immediately after that, an inhibitory signal is sent by the cerebellar cortex to the deep nucleus
Output Signals from the Cerebellum • From the deep nuclei, output signals leave the cerebellum: • A pathway originates in the midline structures (vermis) and to medullary and pontile areas of the brain stem (equlibrium) • A pathway originates in • Intermediate zone • Interposed nucleus • Ventrolateral and ventroanterior portions of the thalamus • Basal ganglia • Red nucleus and reticular formation of the upper brain stem • This pathway helps coordinate reciprocal contractions of agonist and antagonist muscles in the limbs
Output Signals from the Cerebellum • A pathway originates that begins in the cerebellar cortex of the lateral zone, then to dentate nucleus, thalamus and then to the cerebral cortex
Functional Unit of the Cerebellar Cortex • The Purkinje cell and deep nuclear cell • Afferent input is carried by climbing fibers and mossy fibers • The output from the functional unit is from the deep nuclear cell • This is under both excitatory and inhibitory influences
Functional Unit of the Cerebellar Cortex • The Purkinje cells and deep nuclear cells fire continuously under normal resting conditions • Balance between excitation and inhibition at the deep cerebellar nuclei • Other inhibitory cells in the cerebellum: basket and stellate cells in the cerebellum provide additional inhibitory signals • Their role in lateral inhibiton • Turn-On/Turn-Off and Turn-Off/Turn-On output signals from the cerebellum: typical function of the cerebellum is to provide rapid turn-on signals for the agonist muscles and simultaneous reciprocal turn-off signals for the antagonist muscles
Functional Unit of the Cerebellar Cortex • The Purkinje cells learn to correct motor errors: role of climbing fibers • Timing and force of muscle contractions must be learned by the cerebellum • Failure of actual movement to match the intended movement at first attempt
Function of the cerebellum in overall motor control • The nervous system uses the cerebellum to coordinate motor control functions at three levels: • Vestibulocerebellum: it provides neural circuits for body’s equlibrium movements • Spinocerebellum: It provides circuitry for coordinating movements of mainly distal limbs • Cerebrocerebellum: Lateral portions of the cerebellum, signal transduction with the cerebral cortex
Functional Divisions-cerebellum • Vestibulocerebellum (flocculonodular lobe)
The vestibulocerebellum • input-vestibular nuclei • output-vestibular nuclei
The vestibulocerebellum • Function: • The control of the equilibrium and postural movements. • Especially important in controlling the balance between agonist and antagonist M. contractions of the spine, hips, and shoulders during rapid changes in body positions. Method • Calculate the rates and direction where the different parts of body will be during the next few ms. • The results of these calculations are the key to the brains’s progression to the next sequential movement.
Spinocerebellum (vermis & intermediate) • input-periphery & spinal cord: • output-cortex
Spinocerebellum (vermis & intermediate) Functions: -- Provide the circuitry for coordinating mainly the movements of the distal portions of the limbs, especially the hands and fingers -- Compared the “intentions ” from the motor cortex and red nucleus, with the “performance” from the peripheral parts of the limbs, --Send corrective output signals to the motor neurons in the anterior horn of spinal cord that control the distal parts of the limbs (hands and fingers) --Provides smooth, coordinate movements of the agonist and antagonist M. of the distal limbs for the performance of acute purposeful patterned movements.
Cerebellar Control of Ballistic Movements • Sequential control of rapid movements, such as movements of the fingers in typing • Or saccadic movements of the eyes when reading • When the cerebellum is removed, these changes occur in ballistic movements: • Movements are slow to develop • The force is weak • Movements are slow to turn off (intentional tremor) • Biphasic nature of ballistic movements: first excitatory and then delayed inhibitory function is required
Cerebrocerebellum (lateral zone) input-pontine N. output-premotor cortex and primary and association somatosensory areas (no direct output to the primary motor area)
Cerebrocerebellum (lateral zone) • Receives all its input from the motor cortex, adjacent pre-motor and somatic sensory cortices of the brain. Transmits its output information back to the brain. • Functions in a “feedback” manner with all of the cortical sensory-motor system to plan sequential voluntary body and limb movements, • Planning these as much as tenths of a second in advance of the actual movements (mental rehearsal of complex motor actions)
Vestibulocerebellum (flocculonodular lobe) • Balance and body equilibrium • Spinocerebellum (vermis & intermediate) • Rectify voluntary movement • Cerebrocerebellum (lateral zone) • Plan voluntary movement
Clinical Abnormalities of the Cerebellum • Failure of progression: • Dysdiadochokinesia: When the motor system fails to predict where the different parts of the body will be at a given time, it loses perception of the parts during motor movement • Succeeding movement may begin too early or much too late • Dysarthria: Failure of orderly succession of individual mucle movements in talking • Intention tremor (or action tremor) • Cerebellar nystagmus • Hypotonia
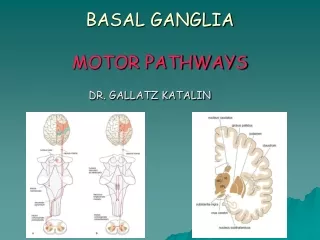
The motor functions of basal ganglia Caudate nucleus, Putamen, Globus Pallidus, Substantia Nigra and Subthalamic Nucleus
Neuronal Circuitry of the Basal Ganglia Putamen circuit Caudate circuit
Basal Ganglia Connections • Circuit of connections • cortex to basal ganglia to thalamus to cortex • Helps to program automatic movement sequences (walking and arm swinging or laughing at a joke) • Output from basal ganglia to reticular formation • reduces muscle tone • damage produces rigidity of Parkinson’s disease
The Putamen Circuit • One of the principal roles of the basal ganglia in motor control is to function in association with the corticospinal system to control complex patterns of motor activity • Writing letters of alphabet • Cutting paper with scissors, hammering nails, most aspects of vocalization and any other skilled movements • Neural pathways of the putamen circuit: • Beginning in premotor and supplementary areas of motor cortex and somatosensory areas of the cortex • Putamen • Internal portion of the globus pallidus • Ventoanterior and ventrolateral relay nuclei of the thalamus • And then back to the primary motor cortex and supplementary cerebral areas associated with the primary motor cortex
Abnormal function of the putamen circuit • Athetosis: continuous writhing movements of hands, arms, neck or the face • Hemiballismus: A lesion in the subthalamus often leads to sudden unilateral wild, large amplitude flinging movements of the arm and leg, normally causing falls and preventing postural maintenance • Chorea • Parkinson’s disease
The Caudate Circuit • Role of basal ganglia for cognitive control of sequences of motor patterns • The caudate nucleus plays a major role in cognitive control of motor activity • The caudate nucleus receives large amounts of its input from the assoaiction areas of the cerebral cortex processing different types of sensory and motor information into usable thought patterns • Cognitive functions and rapid control of motor activity
Components of Basal Ganglia Caudate Putamen GPe 1. Corpus Striatum Striatum ----- Caudate Nucleus & Putamen Pallidum ----- Globus Pallidus (GP) GPi
Components of Basal Ganglia 2. Substantia Nigra Pars Compacta (SNc) Pars Reticulata (SNr) STN 3. Subthalamic Nucleus (STN) SN (r & c)
Function of the basal ganglia to change the timing and to scale the intensity of movements • To determine how rapidly the movement is to be performed • To control how large the movement will be • In patients with severe lesions of the basal ganglia, these timing and scaling of the movements are poor
Functions of Specific Neurotransmitter Substances in the Basal Ganglial System • Dopamine pathways from SN to caudate nucleus and putamen • GABA pathways from the caudate nucleus and putamen to the globus pallidus and SN • ACh pathways from the cortex to the caudate nucleus and putamen • Multiple general pathways from the brain stem: • Norepinephrine • Serotonin • Enkephalin • Glutamate
Functions of Specific Neurotransmitter Substances in the Basal Ganglial System
Clinical Syndromes Resulting from Damage to the Basal Ganglia • Aside from athetosis and hemiballismus • Parkinson’s disease • Huntington’s disease (chorea)
Parkinson’s Disease PD Disease of mesostriatal dopaminergic system normal Muhammad Ali in Atlanta Olympic
Parkinson’s Disease Substantia Nigra, Pars Compacta (SNc) DOPAminergic Neuron Clinical Feature (1) Slowness of Movement - Difficulty in Initiation and Cessation of Movement
Parkinson’s Disease Clinical Feature (2) Resting Tremor Parkinsonian Posture Rigidity-Cogwheel Rigidity
HUNTINGTON’S CHOREA Clinical Feature - Predominantly autosomal dominantly inherited chronic fatal disease (Gene: chromosome 4) - Insidious onset: Usually 40-50 - Choreic movements in onset - Frequently associated with emotional disturbances - Ultimately, grotesque gait and severe dysarthria, progressive dementia ensues. Principal Pathologic Lesion: Corpus Striatum (esp. caudate nucleus) and Cerebral Cortex
HEMIBALLISM Clinical Feature - Usually results from CVA (Cerebrovascular Accident) involving subthalamic nucleus - sudden onset - Violent, writhing, involuntary movements of wide excursion confined to one half of the body - The movements are continuous and often exhausting but cease during sleep - Sometimes fatal due to exhaustion - Could be controlled by phenothiazines and stereotaxic surgery Lesion: Subthalamic Nucleus