Download
1 / 1
10 likes | 174 Views
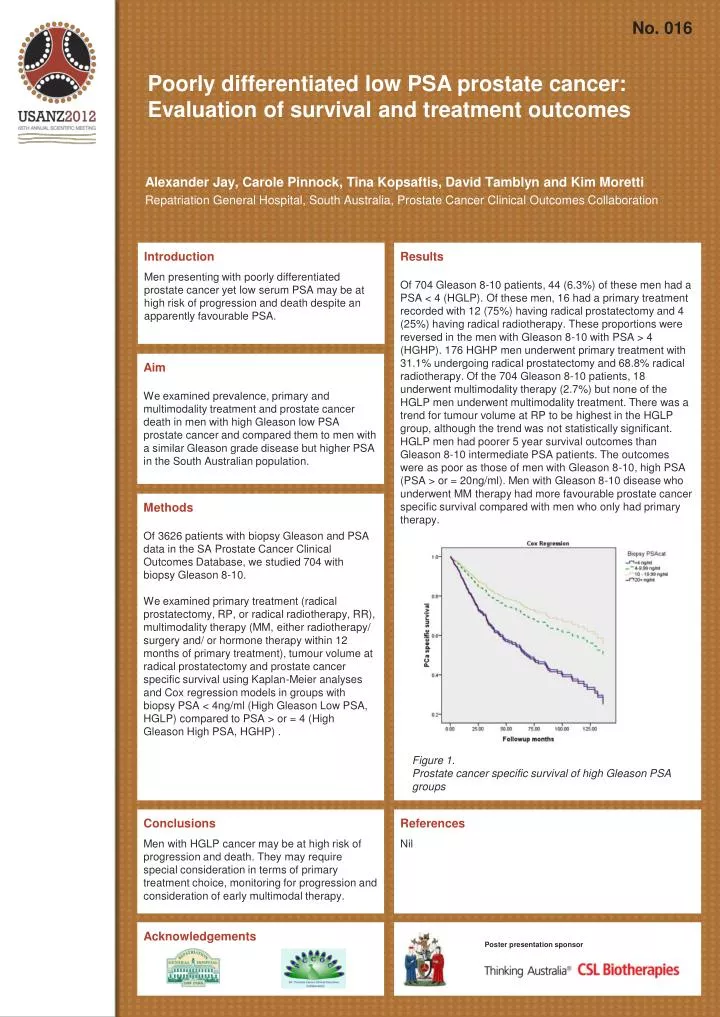
No. 016. Poorly differentiated low PSA prostate cancer: Evaluation of survival and treatment outcomes . Alexander Jay, Carole Pinnock , Tina Kopsaftis , David Tamblyn and Kim Moretti Repatriation General Hospital, South Australia, Prostate Cancer Clinical Outcomes Collaboration.

E N D
No. 016 Poorly differentiated low PSA prostate cancer: Evaluation of survival and treatment outcomes Alexander Jay, Carole Pinnock, Tina Kopsaftis, David Tamblyn and Kim Moretti Repatriation General Hospital, South Australia, Prostate Cancer Clinical Outcomes Collaboration Introduction Men presenting with poorly differentiated prostate cancer yet low serum PSA may be at high risk of progression and death despite an apparently favourable PSA. Results Of 704 Gleason 8-10 patients, 44 (6.3%) of these men had a PSA < 4 (HGLP). Of these men, 16 had a primary treatment recorded with 12 (75%) having radical prostatectomy and 4 (25%) having radical radiotherapy. These proportions were reversed in the men with Gleason 8-10 with PSA > 4 (HGHP). 176 HGHP men underwent primary treatment with 31.1% undergoing radical prostatectomy and 68.8% radical radiotherapy. Of the 704 Gleason 8-10 patients, 18 underwent multimodality therapy (2.7%) but none of the HGLP men underwent multimodality treatment. There was a trend for tumour volume at RP to be highest in the HGLP group, although the trend was not statistically significant. HGLP men had poorer 5 year survival outcomes than Gleason 8-10 intermediate PSA patients. The outcomes were as poor as those of men with Gleason 8-10, high PSA (PSA > or = 20ng/ml). Men with Gleason 8-10 disease who underwent MM therapy had more favourable prostate cancer specific survival compared with men who only had primary therapy. Aim We examined prevalence, primary and multimodality treatment and prostate cancer death in men with high Gleason low PSA prostate cancer and compared them to men with a similar Gleason grade disease but higher PSA in the South Australian population. Methods Of 3626 patients with biopsy Gleason and PSA data in the SA Prostate Cancer Clinical Outcomes Database, we studied 704 with biopsy Gleason 8-10. We examined primary treatment (radical prostatectomy, RP, or radical radiotherapy, RR), multimodality therapy (MM, either radiotherapy/ surgery and/ or hormone therapy within 12 months of primary treatment), tumour volume at radical prostatectomy and prostate cancer specific survival using Kaplan-Meier analyses and Cox regression models in groups with biopsy PSA < 4ng/ml (High Gleason Low PSA, HGLP) compared to PSA > or = 4 (High Gleason High PSA, HGHP) . Figure 1. Prostate cancer specific survival of high Gleason PSA groups Conclusions Men with HGLP cancer may be at high risk of progression and death. They may require special consideration in terms of primary treatment choice, monitoring for progression and consideration of early multimodal therapy. References Nil Acknowledgements Poster presentation sponsor