Download
1 / 24
410 likes | 1.62k Views
Chlamydia trachomatis , Mycoplasma , Ureaplasma , and other Non- Gonococcal urethritis:. Chlamydia trachomatis: Microscopy and culture: Small unicellular round-to-ovoid bacteria that cannot stained by Gram’s stain.

E N D
Chlamydia trachomatis, Mycoplasma, Ureaplasma, and other Non-Gonococcal urethritis: Chlamydia trachomatis: Microscopy and culture: Small unicellular round-to-ovoid bacteria that cannot stained by Gram’s stain. Someinclusion bodies retain Iodine or the counter stain safranin. Rigid Cell wall . The cell envelope has two lipid bilayers with cell wall material (butnot peptidoglycan nor muramic acid).
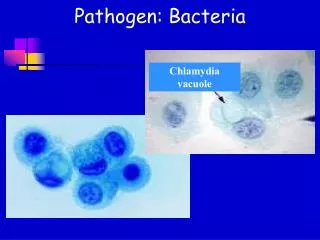
n Obligatory intracellular parasite. It depends on the host cellular energy compounds ATP, and NAD. Cultivated in yolk sac of embryonated egg or tissue culture. Chlamydia inclusion :R. bodies. Chlamydia inclusion .
Pathogenesis and life cycle: -Transmission: Sexual route. -Infectiouspart: The elementary body. -The elementary bodies taken by phagocytosis into susceptible host cell (Columnar epithelial cells). -Once inside the cell, the elementary body prevents fusion of the phagosome and lysosomes. -It will converted into metabolically active dividing Reticulate body. (non-infectious body). -Inclusion bodies. -After 48 hours, rupture of infected cell to release many elementary bodies. -Host cell death, and infection of another cell.
Tissue damage induced by Chlamydia trachomatis: 1-Nongonococcal urethritis: -Caused by: Serovars: D,E, F,.., to K. - In male : Urethritis, infection could extend to epididymitis and prostatitisbut rarely to testicles; (Orchitis: very rare). -One-third of patients have Reiter Syndrome (HLA-B27); Acute aseptic arthritis and urethritis. - In Female: Cervicitis and Pelvic inflammatory disease: Endometritis, Salpingitis. -Exposure to Antibiotics or Interferone-Gamma results in persistence infection. - Tubal factor infertility and Ectopic pregnancy.
N 2-Lymphogranuloma venereum:(LGV): more invasive infection -Caused by Serovars: L1, L2, and L3. -Enters small skin breaks of external genitalia. -Papules in the external genitalia.(for one to two months). -Herpetic-like Ulcer of genitalia. -More invasive infection. -Painfulswelling of inguinal and perirectallymphnodes. - Lymphatic Obstruction; Elephantiasis of Genitalia.
Clinical picture of Chlamydia trachomatis: Urethral discharge : (more mucoid with fewer pus cell). Chlamydial Cervicitis.
Diagnosis of Chlamydia trachomatis infection: Clinical specimens: Urethral discharge, HVS, urine, and Scraping of infected epithelial cells or Squamocolumnar junction swabs. 1- Direct microscopy: A-Immunofluorescent microscopy. B-Electron microscopy. 2-Detection of Chlamydia genetic material by PCR. 3-Serology: Serologic testing for specific antibodies is not helpful except in suspected Lymphogranulomavenereum. 4-Antibiotic sensitivity: Doxycycline, azithromycin, and Erythromycin.
Laboratory diagnosis: Immunofluorescent staining of inclusion body. Electron microscopy and immuno-electrone microscopy for inclusions.
Mycoplasma hominis, Mycoplasma genitalium, andUreaplasma urealyticum: The smallest prokaryotic microbe capable of growth on cell-free media. Because of their extremely small size (0.1-0.3 micrometer), Mycoplasma species pass through sterilization filters. Lacking cell walls, all species are enclosed instead by lipid bilayer membrane containing sterols. Due to the absence of Cell walls (No peptidoglycan cell wall): 1-The bacteria are plastic, pleomorphic in nature, and cannot be classified as either coccinor bacilli. 2-The bacteria are resistance to penicillin and cephalosporins.
n Double-stranded DNA genomes measure less than one million Kilodaltons. Cultural characteristics and colony morphology: Facultative anaerobes, and some species are strict anaerobes. Fastidious for external source of cholesterol (serum). Given appropriate supplementation, they can be grown in cell-free media. Colonies are visualized microscopically by 30 to 100 x magnification. Colonies show a characteristics (fried egg) appearance.
Biochemical activities of Mycoplasma and Ureaplasma: -Mycoplasma hominis and Ureaplasma urealyticum grow more rapidly than Mycoplasma pneumoniae. -They can be distinguished by their carbon utilization patterns; -M. hominis degrades arginine. -U. urealyticum hydrolyses urea; ammonia can destroy the epithelial cells. In female: -The major clinical condition associated with M. hominis is postabortal fever. -M. hominis is recovered locally in cases of Pelvic inflammatory disease. -All M. hominis species are Erythromycin resistance.
n Ureaplasma urealyticum and Mycoplasma genitaliumare associated with cases of PID; Endometritis and vaginosis. - Tetracycline is the drug of choice for treatment of M. hominisinfection. - Other species are sensitive to azithromycin. In male: Ureaplasma urealyticum and Mycoplasma genitalium are associated with cases of Urethritis. The infection could be disseminated to other tissue in immunocompromised patients.
Bacterial vaginosis and PID: -The most common vaginal infection worldwide. -Disruption of vaginal normal flora (Lactobacillus species). -Causative agents: 1-Gardnerellavaginalis. Gram-variable-staining facultative anaerobic Coccobacilli. 2-Mycoplasma species or other bacterium. -Other causes of vaginal infection: -Fungal infection: Candidiasis. -Protozoan infection.
Vaginal Candidiasis: -Most commonly encountered opportunistic mycoses worldwide. -Cellular immunity protects against mucocutaneous candidiasis, neutrophils protect against invasive candidiasis -They are members of the normal flora. -More than 150 species of Candida known. -Only ten species cause disease in humans. -The most common species of medical significance are: 1-Candidaalbicans. 2-Candidatropicalis.
Morphology and cultural characteristics: Candidais thin-walled, small yeasts (4 to 6 microns) that reproduce by budding. Microscopically: Candida albicansis a dimorphic fungi, in addition to budding yeast cells, pseudohyphae, it also can produce true hyphae. Asexual Germination of Candida occurs by production of Blastosporesor Chlamydiospores.
n -Macroscopically: on agar media they produce creamy colonies within 24 hours at 37 C or room temperature. -Candidaspecies produce a small ,white, rounded colonies with feet projection and regular margin. Germ tube test: -Candida species must be incubated with serum for 90 minutes at 37C; -yeast cells of C. albicanswill produce true hyphae or germ tube.
Clinical presentation of Candida albicans: Candida albicanscauses almost 100% of cases of oropharyngeal candidiasis and at least 90% of cases of Candida vulvovaginitis. Vaginal candidiasis presents as itching and burningpain of the vagina. Thick or thin white discharge. HVS, and discharge should be examined for differential diagnosis. Candida albicans can cause urethritis in male.
Trichomoniasis: (Vaginal and Urethral infection): Trichomonas vaginalis: Classification: Urogenital Mastigophora. Morphology: 20-30 um ,oval or pyriform in shape ,with short undulating membrane , axostyle and four free flagella. Transmission:sexual intercourse, and contaminated clothes. Pathology and Clinical picture: Vaginitis- itching, copious- yellowish offensive discharge. Urethritisin male and female. Prostatitisand seminal vesiculitis in male. Diagnosis:finding the trophozoitein smears from vaginal or urethral discharge.
Congenital and Perinatal infections: Congenital (intrauterine or prenatal) infections are those transmitted during fetal life by transplacental route from mother to fetus. The causative agents are: 1-Cytomegalovirus. 2-Herpes simplex virus. 3-HIV. 4-Parvovirus B19. 5-rubella virus. 6-Treponemapallidum. 7-Toxoplasma gondii.
The effect of intrauterine infection on fetus: Three types of effects on the growing fetus may result from this infections: 1-Abnormal organogenesis: rubella :structural abnormalities in tissue and organs; defects in retina, pulmonary artery stenosis. 2-Inflammatory response results in tissue damage: CMV and T.gondii: cause Cerebritis; so cerebral atrophy and intracranial calcification. 3-Placental insufficiency: low birth weight, premature birth, fetal death.
N Perinatal infections are acquired from mother at birth or during the first four weeks after birth from Maternal or non-maternal sources. Causative agents: 1-E.coli and other Enterobacteriaceae. 2-Group B Streptococci. 3-Listeriamonocytogenes. 4-Gonococci and Chlamydia 5-Viruses and Candida. Effects: Bacterial sepsis: Mortality rate is 10-40%. Meningitis: Significant neurological damage: in 20-50% of survivors.