SMC Evaluation Programme
SMC Evaluation Programme. Overview. Context Evaluation Programme Stakeholders SMC advice Conclusions. Context. SMC established October 2001 SMC first advice April 2002 Remit

SMC Evaluation Programme
E N D
Presentation Transcript
Overview • Context • Evaluation Programme • Stakeholders • SMC advice • Conclusions
Context • SMC established October 2001 • SMC first advice April 2002 Remit To provide advice to NHS boards and their ADTCs across Scotland about the status of all newly licensed medicines, all new formulations of existing medicines and new indications for established products
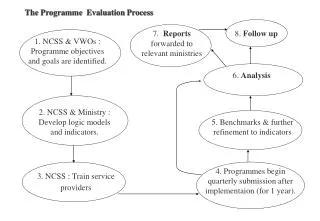
Assessment process Patient group Pharmacy assessment Team NDC SMC Proforma Health Economics group Company response Submitted by company Critical Appraisal of submission Scientific Advisory Committee Advice in context of NHS Scotland
Evaluation Programme • Stakeholders • SMC advice
Programme Delivery • Structure • Project Team • Management Group • Reference Group • SMC Executive Team • Timescale • 2 year programme (April 06 - March 08)
Stakeholders – methods 1Impact on ADTCs role and function • 2000 • 2002 • 2003/4 • 2006/7 Review of Public information • Workshop June 2007 ADTCs n~ 60 + +
Stakeholders – methods 2Engagement with stakeholders Public Partners* Postal questionnaires and interviews (n=154) Pharmaceutical Industry Workshop (n~100) ADTCs Workshop (n~60) + + * ScotCen – Scottish Centre for Social Research
Stakeholders - Key FindingsImpact on ADTCs’ role and function
SMC Advice – method 1 Medicine Profiles ( n=74) • Not Recommended - 20/57 (35%) • Accepted / Restricted – 54/149 (36%)
SMC Advice – method 2 • Case study – Etanercept • Medicine use in psoriatic arthritis • Implementation of SMC Etanercept Protocol (Aug 2006) • Budget Impact • Compare estimate and actual spend (n=28) • Focus group to understand how NHS boards use this information
SMC Advice – Key FindingsNot Recommended advice (n=20) • 65% of advice issued within 6months of medicine launch date • Use before SMC advice (n=20) • £1.4m ( context - £3.7billion) • Use after SMC advice 2005/6 (n=10) • £1m ( 0.1% of drugs bill )
Variation in advice issued by national bodies to NHS boards and clinicians
Lack of engagement of relevant clinical experts in early stages of SMC
SMC Advice - Key FindingsSMC accepted/restricted advice (n=54) • 81% of advice issued within 6 months • Use before SMC advice ( n=41) • £1m (context £3.7billion) • Insufficient robust data for hospital medicines
updateSMC Advice - Key FindingsSMC accepted/restricted advice (n=54)
SMC Advice - Key FindingsEtanercept Table 1: SMC etanercept protocol – Adherence of NHS boards in Scotland at August 2006
SMC advice - Key Findings Budget Impact • Reliability of budget impact estimates • Unable to meaningfully compare data due to series of factors Experience of NHS Boards’ use of information • Budget information valued by NHS Boards for local planning • Further clarity and definition required to improve quality
Conclusions - Successes • ADTCs have adapted and evolved in response to SMC • SMC has good engagement with ADTCs and Pharmaceutical Industry • Budget impact information is valued by NHS boards
Conclusions – Challenges • Effective engagement with public partners remains a challenge • Monitoring use of medicines is limited by availability of robust hospital medicines data and lack of patient level data
Conclusion – Future Direction • Actions based on the factors identified which help to explain medicine use • Development of a more consistent approach to budget impact estimates • Actions based on findings from public partners • Continued development of effective methodologies to assess the contribution of HTA organisations to patient care
Acknowledgements The project team Marion Bennie Laura McIver Sharon Hems Bill Ramsay Samuel Oduro Vicky Cairns Corri Black Joy Nicholson Rupert Payne
Acknowledgements • SMC Evaluation Reference and Management Groups • SMC (User Group / PAPIG) • SMC (Economic / Admin / Exec Team) • ADTCs and clinical networks • ABPI • Information Services Division staff, NSS • ScotCen / Scott Hill • Sue Hewitt • NHS QIS Comms team