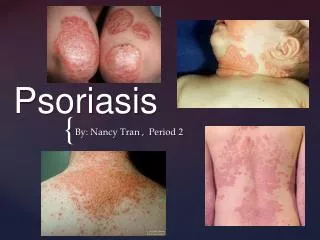
Psoriasis
Psoriasis. Medical Student Core Curriculum in Dermatology. Last updated March 28, 2011. Module Instructions.

Psoriasis
E N D
Presentation Transcript
Psoriasis Medical Student Core Curriculum in Dermatology Last updated March 28, 2011
Module Instructions • The following module contains a number of blue, underlined terms which are hyperlinked to the dermatology glossary, an illustrated interactive guide to clinical dermatology and dermatopathology. • We encourage the learner to read all the hyperlinked information.
Goals and Objectives • The purpose of this module is to help medical students develop a clinical approach to the evaluation and initial management of patients presenting with psoriasis. • By completing this module, the learner will be able to: • Identify and describe the morphology of psoriasis • Describe associated triggers or risk factors for psoriasis • Describe the clinical features of psoriatic arthritis • List the basic principles of treatment for psoriasis • Discuss the emotional and psychosocial impact of psoriasis on patients • Determine when to refer a patient with psoriasis to a dermatologist
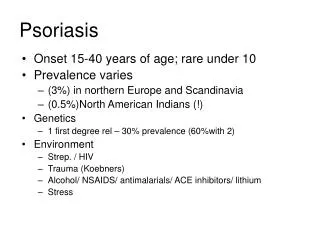
Psoriasis: The Basics • Psoriasis is a chronic multisystem disease with predominantly skin and joint manifestations • Affects approximately 2% of the U.S. population • Age of onset occurs in two peaks: ages 20-30 and ages 50-60, but can be seen at any age • There is a strong genetic component • About 30% of patients with psoriasis have a first-degree relative with the disease • Waxes and wanes during a patient’s lifetime, is often modified by treatment initiation and cessation and has few spontaneous remissions
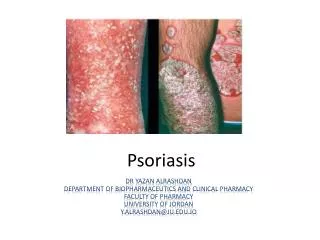
Classification of Psoriasisis based on morphology • Plaque: scaly, erythematous patches, papules, and plaques that are sometimes pruritic • Inverse/Flexural: lesions are located in the skin folds • Guttate: presents with drop lesions, 1-10mm salmon-pink papules with a fine scale • Erythrodermic: generalized erythema covering nearly the entire body surface area with varying degrees of scaling • Pustular: clinically apparent pustules
Classification of Psoriasisis based on morphology (cont.) • Pustular psoriasis includes: • Rare, acute generalized variety called “von Zumbusch variant” • Palmoplantar – localized involving palms and soles • Clinical findings in patients frequently overlap in more than one category • Different types of psoriasis may require different treatment
What Type of Psoriasis? A B C D
Guttate Psoriasis • Acute onset of raindrop-sized lesions on the trunk and extremities • Often preceded by streptococcal pharyngitis
Inverse/Flexural Psoriasis • Erythematous plaques in the axilla, groin, inframammary region, and other skin folds • May lack scale due to moistness of area
Pustular Psoriasis • Characterized by psoriatic lesions with pustules. • Often triggered by corticosteroid withdrawal. • When generalized, pustular psoriasis can be life-threatening. • These patients should be hospitalized and a dermatologist consulted.
Palmoplantar Psoriasis • May occur as either plaque type or pustular type. • Often very functionally disabling for the patient. • The skin lesions of reactive arthritis typically occur on the palms and soles and are indistinguishable from this form of psoriasis.
Psoriatic Erythroderma • Involves almost the entire skin surface; skin is bright red • Associated with fever, chills, and malaise • Like pustular psoriasis, hospitalization is sometimes required See the module on Erythroderma for more information
Question • How would you describe these lesions? • What type of psoriasis does this patient have?
Plaque Psoriasis • Well-demarcated plaques with overlying silvery scale and underlying erythema • Chronic plaque psoriasis is typically symmetric and bilateral • Plaques may exhibit: • Auspitz sign (bleeding after removal of scale) • Koebner phenomenon (lesions induced by trauma)
Plaque Psoriasis: The Basics • Plaque psoriasis is the most common form, affecting 80-90% of patients • Approximately 80% of patients with plaque psoriasis have mild to moderate disease – localized or scattered lesions covering less than 5% of the body surface area (BSA) • 20% have moderate to severe disease affecting more than 5% of the BSA or affecting crucial body areas such as the hands, feet, face, or genitals
Psoriasis: Pathogenesis • Psoriasis is a hyperproliferative state resulting in thick skin and excess scale • Skin proliferation is caused by cytokines released by immune cells • Systemic treatments of psoriasis target these cytokines and immune cells
Case One Mr. Ronald Gilson
Case One: History • HPI: Mr. Gilson is a 24-year-old man who presents with a red lesion around his belly button that has been present for one month with occasional itching. • He has been reading on the internet and asks: “Do I have psoriasis?”
Case One, Question 1 • What elements in the history are important to ask when considering the diagnosis of psoriasis? • Family history • Medications • Recent illnesses / Past medical history • Social history • All of the above
Case One, Question 1 Answer: e • What elements in the history are important to ask when considering the diagnosis of psoriasis? • Family history • Medications • Recent illnesses / Past medical history • Social history • All of the above
Ask About Past Medical History • Psoriasis can be triggered by infections, especially streptococcal pharyngitis • Psoriasis can be more severe in patients with HIV • Up to 20% of psoriasis patients have psoriatic arthritis, which can lead to joint destruction • There is a positive correlation between increased BMI and both prevalence and severity of psoriasis • Patients with psoriasis may have an increased risk for cardiovascular disease and should be encouraged to address their modifiable cardiovascular risk factors
Ask About Medication History • Psoriasis can be triggered or exacerbated by a number of medications including: • Systemic corticosteroid withdrawal • Beta blockers • Lithium • Antimalarials • Interferons
Ask About Family History • There is a strong genetic predisposition to developing psoriasis • 1/3 of psoriasis patients have a positive family history • However, this means up to 2/3 of patients with psoriasis do not have a family history of psoriasis, so a negative family history does not rule it out
Ask About Health-Related Behaviors • Studies have revealed smoking as a risk factor for psoriasis • Alcohol consumption is more prevalent in patients with psoriasis and it may increase the severity of psoriasis • A higher BMI is associated with an increased prevalence and severity of psoriasis
Back to Case One Mr. Ronald Gilson Twenty-one year-old man with red lesion around his umbilicus
Case One: History Continued • PMH: no major illnesses or hospitalizations • Medications: none • Allergies: none • Family history: adopted, unknown • Social history: lives with roommates in an apartment, graduate student in physics • Health-related behaviors: no tobacco or drug use, consumes 3-6 beers on weekends • ROS: negative
Psoriasis: Clinical Evaluation • Although you should perform a total body skin exam, plaque psoriasis tends to appear in characteristic locations • Key Areas: scalp, ears, elbows and knees (extensor surfaces), umbilicus, gluteal cleft, nails, and sites of recent trauma • Observation of psoriatic lesions in these locations helps distinguish psoriasis from other papulosquamous (scaly) skin disorders
Back to Case One: Skin Exam • Erythematous plaque around and in the umbilicus • Erythematous plaque with overlying silvery scale is present in the gluteal cleft (gluteal pinking)
Differential Diagnosis of Psoriasis • Mr. Gilson is given a diagnosis of psoriasis based on the clinical evaluation • Psoriasis is typically diagnosed on clinical exam because of its characteristic location and appearance • Other conditions to be considered in the patient with chronic plaque psoriasis are: • Tinea corporis • Nummular eczema • Seborrheic dermatitis • Secondary syphilis • Drug eruption
Case Two Mr. Bruce Laney
Case Two: History • HPI: Mr. Laney is a 68-year-old man with a history of psoriasis who presents with increased joint pain and joint changes. He currently uses a topical steroid to treat his psoriasis. • PMH: psoriasis x 40 years, hypertension x 20 years • Medications: topical clobetasol for psoriasis, hydrochlorothiazide for blood pressure • Allergies: none • Family history: mother and father both had psoriasis • Social history: lives with his wife in a house, retired • ROS: negative
Large erythematous plaque with overlying silvery scale on anterior scalp Case Two: Skin Exam
Case Two: Skin Exam • Erythematous plaque with overlying silvery scale at the external auditory meatus and behind the ear • Also with nail pitting
Case Two: Exam Continued • Erythematous and edematous foot, with dactylitis (sausage digit) of the 2nd digit, and destruction of the DIP joints • Onychodystrophy: nail pitting and onycholysis
Case Two, Question 1 • Mr. Laney has psoriasis complicated by psoriatic arthritis. What part(s) of his history/exam are most characteristic of a patient with psoriatic arthritis? • History of extensive psoriasis • Presence of nail pitting • Use of clobetasol • All of the above
Case Two, Question 1 Answer: b • Mr. Laney has psoriasis complicated by psoriatic arthritis. What part(s) of his history/exam is most consistent with this diagnosis? • History of extensive psoriasis • Presence of nail pitting (up to 90% of patients with psoriatic arthritis may have nail changes) • Use of clobetasol • All of the above
Psoriatic Onychodystrophy • Nail psoriasis can occur in all psoriasis subtypes • Fingernails are involved in ~ 50% of all patients with psoriasis. • Toenails in 35% • Changes include: • Pitting: punctate depressions of the nail plate surface • Onycholysis: separation of the nail plate from the nail bed • Subungual hyperkeratosis: abnormal keratinization of the distal nail bed • Trachyonychia: rough nails as if scraped with sandpaper longitudinally
Psoriatic Arthritis (PsA) • Arthritis in the presence of psoriasis • A member of the seronegativespondyloarthropathies • Symptoms can range from mild to severe • Occurs in 10-25 percent of patients with psoriasis • Can occur at any age, but for most it appears between the ages of 30 and 50 years • It is NOT related to the severity of psoriasis • Five clinical patterns of arthritis occur • Most common is oligoarthritis with swelling and tenosynovitis of one or a few hand joints • Flares and remissions usually characterize the course of psoriatic arthritis
Psoriatic Arthritis Continued • Health care providers are encouraged to actively seek signs and symptoms of PsA at each visit • PsA may appear before the diagnosis of psoriasis • If psoriatic arthritis is diagnosed, treatment should be initiated to: • Alleviate signs and symptoms of arthritis • Inhibit structural damage • Maximize quality of life • Diagnosis is based on clinical judgment • Specific patterns of joint inflammation, absence of rheumatoid factor, and the presence of skin and nail lesions of psoriasis aid clinicians in making the diagnosis of PsA
More Examples of PsA Desquamation of the overlying skin as well as joint swelling and deformity (arthritis mutilans) of both feet Swelling of the PIP joints of the 2-4th digits, DIP involvement of the 2nd digit
Case Three Ms. Sonya Hagerty
Case Three: History • HPI: Ms. Hagerty is an 18-year-old healthy woman with a new diagnosis of psoriasis. She reports lesions localized to her knees with no other affected areas. She has not tried any therapy. • PMH: no major illnesses or hospitalizations • Medications: occasional multivitamin • Allergies: none • Family history: noncontributory • Social history: lives in the city with her parents and attends high school • Health-related behaviors: no tobacco, alcohol, or drug use • ROS: slight pruritus
Case Three: Skin Exam • Erythematous plaques with overlying silvery scale on the extensor surface of the knee.
Case Three, Question 1 • Which of the following would you recommend to start treatment for Ms. Hagerty’s psoriasis? • Biologic (immunomodulators) • High potency topical steroid • Low potency topical steroid • Systemic steroids • Topical antifungal
Case Three, Question 1 Answer: b • Which of the following would you recommend to start treatment for Ms. Hagerty’s psoriasis? • Biologic (immunomodulators) • High potency topical steroid • Low potency topical steroid • Systemic steroids • Topical antifungal
Psoriasis: Treatment • Since the psoriasis is localized (less than 5% body surface area), topical treatment is appropriate • First line agents: high potency topical steroid in combination with calcipotriene (vitamin D analog) • Other topical options: tazarotene, salicylic or lactic acid, tar, calcineurin inhibitors
Psoriasis: Treatment • Factors that influence type of treatment: • Age • Type of psoriasis: • plaque, guttate, pustular, erythrodermic psoriasis • Site and extent of psoriasis: • localized = <5% of BSA • generalized = diffuse or >30% involvement • Previous treatment • Other medical conditions