Download
1 / 72
720 likes | 735 Views
Section of Spinal cord Clinical correlation. 三總神經科部 宋岳峰醫師 March 10, 2014. Introduction. Extends from the foramen magnum where it is continuous with the medulla to the level of the first or second lumbar vertebrae 40 to 50 cm long and 1 cm to 1.5 cm in diameter

E N D
Section of Spinal cordClinical correlation 三總神經科部 宋岳峰醫師 March 10, 2014
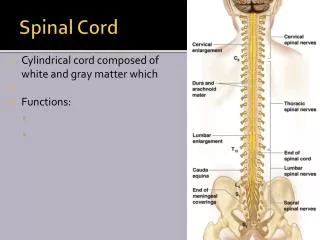
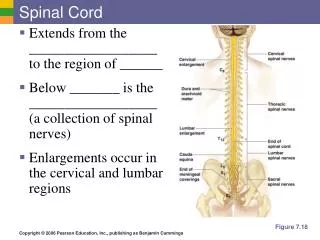
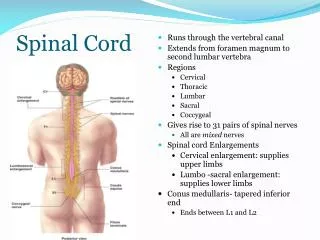
Introduction • Extends from the foramen magnum where it is continuous with the medulla to the level of the first or second lumbar vertebrae • 40 to 50 cm long and 1 cm to 1.5 cm in diameter • Two consecutive rows of nerve roots emerge on each of its sides. These nerve roots join distally to form 31 pairs of spinal nerves
There are 31 segments, defined by 31 pairs of nerves exiting the cord 8 cervical 12 thoracic 5 lumbar 5 sacral 1 coccygeal nerve Dorsal and ventral roots enter and leave the vertebral column respectively through intervertebral foramen at the vertebral segments corresponding to the spinal segment Coccygeal
General Features • Carry sensory information from the body and some from the head to the central nervous system (CNS) via afferent fibers • Motor neurons in the ventral horn project their axons into the periphery to innervate skeletal and smooth muscles • Mediate autonomic control for most of the visceral functions
Cross immediately (or sometimes first travels up one or two segments in the cord); therefore contralateral ANTEROLATERAL SYSTEM (spinothalamic tract): PAIN TEMPERATURE CRUDE TOUCH
Travels ipsilaterally in the cord and crosses in the medulla DORSAL COLUMN - MEDIAL LEMNISCUS PATHWAY : DISCRIMINATIVE TOUCH JOINT POSITION VIBRATION
Corticospinal Tract: Carries motor commands from the brain 80% decussate to lateral corticospinal tract 20% continue ipsilaterally as the medial corticospinal tract
High C-spine • Usually associated with trauma - Atlas ring burst (diving), C2 pedicle fracture with subluxation - Involves quadriparesis and respiratory failure (phrenic nerve: C3, C4, C5)
Low C-spine • Biceps weakness: C5, C6 • Triceps, wrist extensors, and pronator weakness: C7 • Hand weakness: C8, T1 • Sensory loss over arms
Thoracic spine • High thoracic spine and low C-spine have sympathetic nervous system involvement (hypotension, bradycardia, Horner’s syndrome) • Sensory level found along the trunk • Some degree of weakness in the leg
Horner’s syndrome • Miosis • Ptosis • Anhydrosis
Lumbar spine • Weakness in the legs • Sensory changes in the legs and saddle area • Conus medullaris: bowel/bladder involvement
Cauda equina • Lower motor signs of flaccidity, areflexia and weakness but with bowel/bladder involvement and sensory level in saddle up to L1
Patterns of Sensory Loss Vibration sense Posterior column spinal cord syndrome: B12 deficiency, Friedrich’s ataxia
Patterns of Sensory Loss Pain and temperature Cape Anesthesia Central spinal cord syndrome: Syringomyelia, Intrinsic spinal cord tumor
Patterns of Sensory Loss Pain and temperature, contralateral to lesion Position, vibration sense, ipsilateral to lesion All modalities, at lesion Brown-Sequard Syndrome: Extrinsic spinal cord tumor
Patterns of Sensory Loss All modalities Complete spinal cord transection: trauma, transverse myelitis
Demyelinating disease Tumor Vascular disease Inflammatory disease Infection Spinal cord abnormalities
Demyelinating diseases • Multiple Sclerosis • Transverse Myelitis (TM)
Tumor • Astrocytoma: slowly progressive • Ependymoma, hemangioblastoma • Metastases to the cord are very uncommon
Vascular disease • Distant vascular occlusion or aortic disease with thrombosis, dissection, or surgical clamping • Sometimes with microscopic fragments of herniated nucleus pulposus • Arteriovenous malformations (AVM) may cause ischemia
Anterior cord syndrome • Involve the spinothalamic and corticospinal tracts, giving paresis and loss of pain below the level • Usually associated with cord compression, but also can be seen with infarction of the anterior spinal artery
Inflammatory • Vasculitis
Infection • Herpes zoster: radicular pain with dermatomal eruption
Poliomyelitis: destroys anterior horn cells • Retroviruses HTLV-1 (Tropical spastic paraparesis) and HIV-1 • Neurosyphilis: tabes dorsalis-lancinating pains, dorsal column loss, slapping gait
Degenerative diseases • Amyotrophic lateral sclerosis (ALS) • Spinal muscular atrophy • Friedreich’s ataxia Stephen Hawking suffers from amyotrophic lateral sclerosis
Metabolic diseases • Subacute combined degeneration - Vitamin B12 deficiency leading to demyelination of the posterior columns and spreading secondarily to the corticospinal tract - Some peripheral nerve involvement - Symptoms including paresthesias, loss of vibratory and position sensation, weakness and spasticity of the legs
Case 1 • A 38-year-old woman • Sudden onset of sharp pain at the back of her neck on waking in the morning • Progressive numbness and weakness in her four limbs a few minutes later • Difficulty breathing and urinary retention when she was taken to the ER
No history of trauma, neck pain, fever, skin rash, or recent illness • Medical history is unremarkable • Denied smoking, drinking and use of illicit drugs • No any significant family history