CHROMOSOMAL DISORDERS
CHROMOSOMAL DISORDERS. http://krismendillo.wordpress.com. Chromosome abnormality. Chromosome abnormality.

CHROMOSOMAL DISORDERS
E N D
Presentation Transcript
CHROMOSOMAL DISORDERS http://krismendillo.wordpress.com
Chromosome abnormality • A chromosome anomaly, abnormality, aberration, or mutation is a missing, extra, or irregular portion of chromosomalDNA. It can be from an atypical number of chromosomes or a structural abnormality in one or more chromosomes. • Akaryotype refers to a full set of chromosomes from an individual which can be compared to a "normal" karyotype for the species via genetic testing. • A chromosome anomaly may be detected or confirmed in this manner. Chromosome anomalies usually occur when there is an error in celldivision following meiosis or mitosis. • There are many types of chromosome anomalies. They can be organized into two basic groups, numerical and structural anomalies
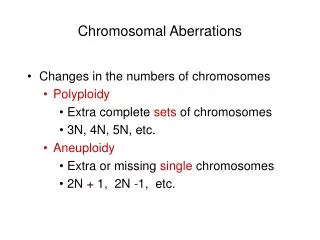
Numerical disorders • This is called aneuploidy (an abnormal number of chromosomes), and occurs when an individual is missing either a chromosome from a pair (monosomy) or has more than two chromosomes of a pair (trisomy, tetrasomy, etc.). • In humans an example of a condition caused by a numerical anomaly is Down Syndrome, also known as Trisomy 21 (an individual with Down Syndrome has three copies of chromosome 21, rather than two). Trisomy has been determined to be a function of maternal age. • An example of monosomy is Turner Syndrome, where the individual is born with only one sex chromosome, an X.
Structural abnormalities • Deletions: A portion of the chromosome is missing or deleted. Known disorders in humans include Wolf-Hirschhorn syndrome, which is caused by partial deletion of the short arm of chromosome 4; and Jacobsen syndrome, also called the terminal 11q deletion disorder. • Duplications: A portion of the chromosome is duplicated, resulting in extra genetic material. Known human disorders include Charcot-Marie-Tooth disease type 1A which may be caused by duplication of the gene encoding peripheral myelin protein 22 (PMP22) on chromosome 17.
Structural abnormalities • Translocations: A portion of one chromosome is transferred to another chromosome. There are two main types of translocations: • Reciprocal translocation: Segments from two different chromosomes have been exchanged. • Robertsonian translocation: An entire chromosome has attached to another at the centromere - in humans these only occur with chromosomes 13, 14, 15, 21 and 22. • Inversions: A portion of the chromosome has broken off, turned upside down and reattached, therefore the genetic material is inverted. • Insertions: A portion of one chromosome has been deleted from its normal place and inserted into another chromosome.
Structural abnormalities • Rings: A portion of a chromosome has broken off and formed a circle or ring. This can happen with or without loss of genetic material. • Isochromosome: Formed by the mirror image copy of a chromosome segment including the centromere. • Chromosome instability syndromes are a group of disorders characterized by chromosomal instability and breakage. They often lead to an increased tendency to develop certain types of malignancies.
Inheritance • Most chromosome abnormalities occur as an accident in the egg or sperm, and therefore the anomaly is present in every cell of the body. Some anomalies, however, can happen after conception, resulting in Mosaicism (where some cells have the anomaly and some do not). • Chromosome anomalies can be inherited from a parent or be "de novo". This is why chromosome studies are often performed on parents when a child is found to have an anomaly. • If the parents do not possess the abnormality it was not initially inherited; however it may be transmitted to subsequent generations.
Cri du chat • Cri du chat syndrome, also known as chromosome 5p deletion syndrome, 5p- (said minus) syndrome or Lejeune’s syndrome, is a rare genetic disorder due to a missing part (deletion) of chromosome 5. • Its name is a French term (cat-cry or call of the cat) referring to the characteristic cat-like cry of affected children. It was first described by JérômeLejeune in 1963. • The condition affects an estimated 1 in 50,000 live births, strikes all ethnicities, and is more common in females by a 4:3 ratio.
Signs and symptoms • The syndrome gets its name from the characteristic cry of affected infants, which is similar to that of a meowing kitten, due to problems with the larynx and nervous system. About 1/3 of children lose the cry by age 2. Other symptoms of cri du chat syndrome may include:
Signs and symptoms • feeding problems because of difficulty swallowing and sucking; • low birth weight and poor growth; • severe cognitive, speech, and motor delays; • behavioral problems such as hyperactivity, aggression, tantrums, and repetitive movements; • unusual facial features which may change over time;
Signs and symptoms • excessive drooling; • small head and jaw; • wide eyes; • skin tags in front of eyes.
Genetics • Cri du chat syndrome is due to a partial deletion of the short arm of chromosome number 5, also called "5p monosomy". • Approximately 90% of cases result from a sporadic, or randomly occurring, de novo deletion. The remaining 10-15% are due to unequal segregation of a parental balanced translocation where the 5p monosomy is often accompanied by a trisomic portion of the genome. • These individuals may have more severe disease than those with isolated monosomy of 5p. A recent study suggests this may not be the case where a trisomy of chromosome 4q is involved.
Genetics • Most cases involve total loss of the most distant 10-20% of the material on the short arm. Fewer than 10% of cases have other rare cytogenetic aberrations (e.g., interstitial deletions,mosaicisms, rings and de novo translocations). The deleted chromosome 5 is paternal in origin in about 80% of de novo cases. • Loss of a small region in band 5p15.2 (cri du chat critical region) correlates with all the clinical features of the syndrome with the exception of the catlike cry, which maps to band 5p15.3 (catlike critical region). The results suggest that 2 noncontiguous critical regions contain genes involved in this condition's etiology. Two genes in these regions, Semaphorine F (SEMA5A) and delta catenin (CTNND2), are potentially involved in cerebral development. • The deletion of the telomerase reverse transcriptase (hTERT) gene localized in 5p15.33 may contribute to the phenotypic changes in cri du chat syndrome as well.
Diagnosis and management • Diagnosis is based on the distinctive cry and accompanying physical problems. Seeing as these symptoms are quite easily observable, affected children are typically diagnosed by a doctor or nurse at birth. • Genetic counseling and genetic testing may be offered to families with individuals who have cri du chat syndrome. Prenatally the deletion of the cri du chat related region in the p arm of chromosome 5 can be detected from amniotic fluid or chorionic villi samples with BACs-on-Beads technology.G-banded karyotype of a carrier is also useful. • Children may be treated by speech, sound, and occupational therapists. Cardiac abnormalities often require surgical correction.
Down syndrome • Down syndrome (DS) or Down's syndrome, also known as trisomy 21, is a genetic disorder caused by the presence of all or part of a third copy ofchromosome 21. • It is typically associated with physical growth delays, characteristic facial features and mild to moderate intellectual disability. • The average IQ of a young adult with Down syndrome is around 50, similar to the mental age of an 8 or 9 year old child.[3]
Down syndrome • Down syndrome can be identified during pregnancy by prenatal screening or after birth by direct observation and genetic testing. Since the introduction of screening, pregnancies with the diagnosis are often terminated.[4][5] Regular screening for health problems common in Down syndrome is recommended throughout the person's life.
Down syndrome • Education and proper care has been shown to improve quality of life. • Some children with Down syndrome are educated in regular school classes while others require more specialized education. • Some children with Down syndrome graduate from high school and in adulthood some individuals work in the community. • The degree of independence possible for an affected individual varies, and some require a more sheltered work environment. • Support in financial and legal matters is often needed. • Life expectancy is around 50 to 60 years in the developed world with proper health care.
Down syndrome • Down syndrome is the most common chromosome abnormality in humans occurring in about 1 per 1000 babies born each year. • It is named afterJohn Langdon Down, the British doctor who fully described the syndrome in 1866. • Some aspects of the condition were described earlier by Jean-Étienne Dominique Esquirol in 1838 and ÉdouardSéguin in 1844.[11] The genetic cause of Down syndrome, an extra copy of chromosome 21, was identified by Dr.JérômeLejeune in 1959.[10]
Signs and symptoms • Those with Down syndrome nearly always have physical and mental disabilities. • As adults their mental abilities are typically similar to that of an 8 or 9 year old. • They also typically have poor immune function and developmental milestones generally are reached at a later age. • There is an increased risk of a number of other health problems including: congenital heart disease, leukemia, thyroid disorders, and mental illness, among others.
Physical • They may have some or all of the following physical characteristics: abnormally small chin, slanted eyes, poor muscle tone, a flat nasal bridge, a single crease of the palm, a protruding tongue due to small mouth, and an enlarged tongue. • Other common features include: a flat and wide face,thereis a short neck, excessive joint flexibility, extra space between big toe and second toe, an abnormal patterns on the fingertops and short fingers. • Instability of the atlanto-axial joint occurs in approximately 20% and may lead to spinal cord injury in 1-2%. • Around half of those with DS haveobstructive sleep apnea.[10] Hip dislocations occur without trauma in an up to a third.
Physical • Growth in height is slower resulting in adults tending to have short stature—the average height for men is 154 cm (5 feet 1 inch) and for women is 142 cm (4 feet 8 inches).[20] Individuals with DS are at increased risk for obesity as they age.[10] There are growth charts specifically for those with Down syndrome.[10]
Neurological • Most individuals with Down syndrome have mild (IQ: 50–70) or moderate intellectual disability (IQ: 35–50) with some cases having severe (IQ: 20–35) difficulties. • As they age they typically perform less well compared to their same aged peers. • Some after 30 years of age may lose their ability to speak. • Those with mosaic Down syndrome typically have scores 10–30 points higher. This syndrome causes about a third of cases of intellectual disability.
Neurological • Fine motor skills[24] and large scale motor skills are often delayed which can interfere with cognitive development. Effects of the condition gross motor skills is variable. Some children will begin walking at around 2 years of age, while others will not walk until age four. • Commonly individuals with Down syndrome have some difficulty speaking with better language understanding.] • 10 to 45% have either stuttering or rapid and irregular speech making them difficult to understand. • They typically do fairly well with social skills. • Behavior problems are not geerallyas great as an issue as in other syndromes associated with intellectual disability.[ • In children with Down syndrome mental illness occurs in nearly 30% with autism occurring in 5-10%. • While generally happy, symptoms of depression and anxiety may develop in early adulthood.
Neurological • Commonly individuals with Down syndrome have some difficulty speaking with better language understanding.10 to 45% have either stuttering or rapid and irregular speech making them difficult to understand. • They typically do fairly well with social skills. • Behaviorproblems are not generally as great as an issue as in other syndromes associated with intellectual disability. • In children with Down syndrome mental illness occurs in nearly 30% with autism occurring in 5-10%.[9] While generally happy, symptoms of depression and anxiety may develop in early adulthood.[3]
Neurological • Children and adults with DS are at increased risk of epileptic seizures which occur in 5-10% of children and up to 50% of adults. • This includes an increased risk of a specific type of seizure called infantile spasms. • Many (15%) who live past 40s develop dementia of the Alzheimer's disease type.[Of those who reach 60 years, 50-70% have the disease.[3]
Senses Brushfield spots, visible in the irises of a baby with Down Syndrome.
Senses • Hearing and vision disorders occur in more than half of people with DS. • Vision problems occur in 38 to 80%.Between 20 and 50% have strabismus, in which the two eyes do not move in tandem. • Refractive errors requiring glasses or contacts are also common. • Cataracts (opacity of the lens) occur in 15%, and may be present at birth. • Keratoconus (thin, cone-shaped corneas), and glaucoma (increased eye pressures) are also more common. • Brushfield spots (small white or grayish/brown spots on the periphery of the iris) are present in 38 to 85%.
Senses • Hearing problems are found in 38-78% of children with Down syndrome compared to 2.5% of normal children. • Diagnosis and aggressive treatment of chronic ear disease (e.g.otitis media) in children with Down syndrome can bring many of the children up to normal hearing levels. • Age related hearing loss of the sensorineural type occurs at a much earlier age affected 10-70%.[3]
Senses • Otitis media with effusion is the most common cause of hearing loss in children with Down's occurring in 50-70%. • Ear infections often start at birth and continue throughout the children's life.[28]The ear infections are mainly due to poor eustachian tubefunction. • However, excessive wax can also cause obstruction of the outer ear canal and hearing problems. Middle ear problems account for 83% of hearing loss in children with Down syndrome. • The degree of hearing loss varies but even a mild degree can have major consequences for speech understanding, language learning, and academics[2] if not detected in time and corrected. • It is important to rule out hearing loss as a contributing factor in social and mental deterioration.
Heart • The rate of congenital heart disease in newborns with Down syndrome is around 40%. • An atrioventricular septal defect also known as endocardial cushion defect is the most common form with up to 40% affected. This is closely followed by ventricular septal defect that affects approximately 35% • Mitral valve problems become common as people age, even in those without heart problems at birth. • Other problems that may occur include: tetralogy of Fallot and patent ductusarteriosus. • People with Down syndrome have a lower risk of hardening of the arteries.
Cancer • Although the general incidence of cancer amongst individuals with Down syndrome is the same as in the general population,thereis a reduced risk of solid cancers and an increased risk of leukemia and testicular cancer. Solid cancers are believed to be less common due to the tumor suppressor genes present on chromosome 21.
Cancer • Cancers of the blood are 10 to 15 times more common in children with DS. • In particular, acute lymphoblastic leukemia is 20 times more common and the megakaryoblastic form of acute myelogenousleukemia is 500 times more common. • Transientmyeloproliferative disease, a disorder of blood cell production that does not occur outside of Down syndrome, affects 3-10% of infants.Thedisorder is typically not serious but occasionally can be. • It resolves most times without treatment; however, in those who have had it there is a 20 to 30 percent risk of developing acute lymphoblastic leukemia at a latter time
Endocrine • Problems of the thyroid gland occur in 20-50%. • Low thyroid is the most common, occurring in almost half of those with DS. Thyroid problems can be due to a poorly or non functioning thyroid at birth (known as congenital hypothyroidism) which occurs in 1%or can develop latter due to an attack on the thyroid by the immune system resulting in Graves disease or autoimmune hypothyroidism. • Type 1 diabetes mellitus is also more common.
Gastrointestinal • Constipation occurs in nearly half of people with DS and may result in changes in behavior. • One potential cause is Hirschsprung's disease, which is due to a lack of nerve cells controlling thecolon, which occurs in 2 to 15%. • Other frequent congenital problems include: duodenal atresia, pyloric stenosis, Meckel diverticulum and imperforate anus. • Celiac disease affects about 7-20% and gastroesophageal reflux disease is also more common
Fertility • Males with Down syndrome usually do not father children, while females have lower rates of fertility relative those who are unaffected. • Fertility is estimated to be present in 30-50% of women and they often have difficulties with miscarriages, premature births, and labor. • Menopause typically occurs at an earlier age.[3] The poor fertility in men is thought to be due to problems with sperm development; however, it may also be related to not being sexually active. • As of 2006 there have been three recorded instances of males with DS fathering children and 26 cases of women having children.Withoutassisted reproductive technologies, approximately half of the pregnancies of someone with Down syndrome will also have the syndrome.
Genetics • Down syndrome is caused by having three copies of the genes on chromosome 21, rather than the usual two. • The parents of the affected individual are typically genetically normal.[ Those who have one child with Down syndrome have about a 1% risk of having a second child with the syndrome, if both parents are found to have normal karyotypes.
Genetics • The extra chromosome content can arise through several different mechanisms. The most common cause (approximately 92-95% of cases) is a complete extra copy of chromosome 21, resulting in trisomy 21. • In 1 to 2.5%, some of the cells in the body are normal and others have trisomy 21, known as mosaic Down syndrome.[41][45] The other common mechanisms that can give rise to Down syndrome include Robertsonian translocation, isochromosomes, ring chromosomee, which contain additional material from chromosome 21. These findings occurs in approximately 2.5% of cases. • Isochromosomes result when the two long arms separate together on one chromosome.
Karyotype • Trisomy 21 (also known by the karyotype 47,XX,+21 for males and 47,XY,+21 for females) is caused by a failure of the chromosomes to separate during egg or sperm development. • As a result, a sperm or egg cell is produced with an extra copy of chromosome 21; this cell thus has 24 chromosomes. • When combined with a normal cell from the other parent, the embryo and baby has 47 chromosomes, with three copies of chromosome 21. Trisomy 21 is the cause of approximately 92 to 95% of cases of Down syndrome, with 88% of cases resulting from non separation of the chromosomes in the mother and 8% coming from non separation in the father.
Translocation • The extra chromosome 21 material may also occur due to a Robertsonian translocation in 2-4% cases.Thismay be a new mutation or previously present in one of the parents. • In this case, the long arm of chromosome 21 is attached to another chromosome, often chromosome 14 known as 45XY,t(14q21q) in males. The risk of this type of Down syndrome is not related to the mothers age.Theparent with such a translocation is usually normal physically and mentally • however, during production of egg or sperm cells there is a higher chance of creating reproductive cells with extra chromosome 21 material.Thisresults in a 15% chance of having a child with DS when the mother is affected and a less than 5% risk if the father is affected.[ • Additionally some children may inherit this translocation while not have DS but are subsequently at higher risk of having children with DS themselves. • In this case it is sometimes known as familial Down syndrome.
Mechanism • In general, extra chromosome 21 DNA leads to an over-expression of certain genes. This over expression is about 50%. • It is estimated that chromosome 21 contains around 310 genes.]\ • Some research has shown that the parts of the chromosome which are of greatest importance are bands 21q22.1-q22.3. • This area includes genes for amyloid, superoxide dismutase, and likely the ETS-2 proto oncogene. • Other research has not confirmed these findings.
Mechanism • The dementia which occurs in Down syndrome is due to too much amyloid beta peptides being produced in the brain. • Senile plaques and neurofibrillary tangles are present in nearly all by 35 years of age even though dementia may not be present. • Those with DS lack a normal number of lymphocytes and produce less antibodies which contributes to there increased risk of infection.[10]
Screening • Guidelines recommend that screening for Down syndrome be offered to all pregnant women, regardless of age. A number of tests can be used, with varying levels of accuracy. They are usually used in combination to increase their detection rate, while maintaining a low false positive rate, but are not definitive.[10] • If screening is positive either amniocentesis or chorionic villous sampling is required to confirm the diagnosis. • Screening in both the first and second trimesters is better than just screening in the first trimester. • The different screening techniques in use are able to pick up 90 to 95% of cases with a false positive rate of between 2 and 5%.