Download
1 / 63
650 likes | 696 Views
Learn about types of nasal airway obstructions such as congenital atresia, trauma-related issues, inflammation/infection, presence of foreign bodies, and neoplastic conditions. Discover diagnostic methods and treatments available.

E N D
MECHANICAL OBSTRUCTION OF AIRWAY DR.dr. BAMBANG UDJI DJOKO RIANTO, SP.THT,M.KES. Referrences: Simpson J.F, Robin I., Ballantyne J.C., Groves J. 1967. A synopsis of otolaryngology. Becker W., Naumann H.H., Pfaltz C.R. 1993. Ear, Nose, and Throat Disease.
CONGENITAL • TRAUMA • INFLAMMATION/INFECTION • NEOPLASM • CORPUS ALIENUM
NOSE ABNORMALITY CONGENITAL MALFORMATIONS • ATRESIA & STENOSIS OF ANTERIOR NARES • - aetiologi: non canalization & non epithelial plug • between the medium & lateral nasal • processes • - incidence: rare • - treatment: the web must be excised
2. ATRESIA POSTERIOR NARES Aetiology: persistence of the primitive bucco- nasal membrane Degrees: - complete unilateral most commonly - incomplete unilateral - complete bilateral - incomplete bilateral • Type or origin • mucous membrane • bony most commonly • mixed
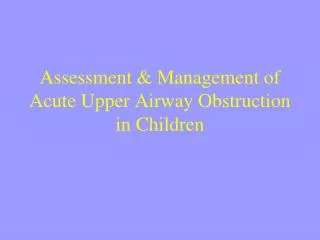
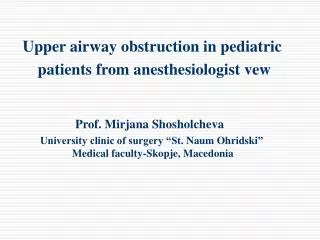
Choanae Tonsilla palatina Epiglottis Aditus laringeus
PATHOLOGY • The partition is attached to: • basis sphenoid, above • medial pterygoid plate of sphenoid • vomer, on the inner side • hard palate, below - The thickened vary from: 1-10 mm
INCIDENCE • neonatal • females are more commonly than male • CLINICAL FEATURES • Unilateral atresia: • - nasal obstruction may not notice for some years • - excessive nasal discharge at /soon after birth • glue like in consistency
Bilateral atresia • - soon after birth • - urgent death from asphyxia • - nasal discharge • - delayed symptom: • - mouth breathing • - failure to develop taste & smell
DIAGNOSIS • rubber catheter or probe can’t be passed • through the nose into nasopharynx (NP) • - posterior rhinoscopy atresia • - radiograph a radiophag substance instilled • into the nose doesn’t reach the NP
TREATMENT - transpalatal excision not for acute emergency case best performed after early childhood - transnasal perforation - simple perforation gauge/burr - emergency procedure in infant - tracheostomy
MAXILLOFACIAL TRAUMA • FRACTURED NASAL BONE • AETIOLOGY • Blows to the front or side of the nose • Nasal obstruction caused by dislocation or • haematoma of the septum • DIAGNOSIS • Clinical examination • crepitation sign • rhinoscopy anterior • radiographic examination
TREATMENT • Reposition of the fracture • Incision of haematom • Anti inflammation
INFLAMMATION/INFECTION • NON SPECIFIC CHRONIC INFECTIVE RHINITIS • caused by inferior turbinate swells (simple type) • - permanent hypertrophic changes cellular infiltration in mucous stroma, glands, blood vessels, lymphatic tissue fibrosis venous & lymphatic obstruction passive oedema nasal polyp
NASAL ALLERGY RHINITIS • - caused by venous stasis of the conchae/mucosa • - nasal polyp • DIAGNOSIS • - symptoms: itching/sneezing, nasal obstruction, rhinorrhea • - careful history family & personal record • clinical examination/rhinoscopy • conchae hypertrophy • nasal discharge
SUPPORTING TEST - eosinophil in nasal discharge - skin test show single or multiple sensitivity - intranasal test (provocation test) TREATMENT -removal of precipitating factors -nasal allergic treatment - Operative nasal polyp
VASOMOTOR RHINITIS • - nasal mucosa is hyperactive to certain stimuli • - the absent of any specific allergic cause • caused by: • - an autonomic imbalance in nasal mucosa • - endocrine imbalance • - septal deflection • - drugs hypotensive drugs • overuse local application • - atmosphere condition • - fume, dust, alcohol
Nasal obstruction caused by: • - hypertrophy of the inferior turbinate • - nasal polyp • TREATMENT • elimination of cause factors • nasal medicament decongestant • cauterization • submucosal diathermy • removal of polyp • psychological adjustment
FOREIGN BODIES IN THE NOSE • more common in children • in adult psychiatry case • - through the anterior nares most commonly • - through the posterior nares food, enter during • an attack of vomiting • - through penetrating wound • - organic or inorganic
CLINICAL FEATURE • unilateral nasal discharge & obstruction • nose bleeding may occur • sneezing • foreign body
DIAGNOSIS - clinical/rhinoscopy examination TREATMENT - removal foreign body
RHINOLITH - nasal concretions formed round a foreign bodies, blood, or mucous AETIOLOGY -foreign bodies exogenous (commonest cause) -blood-cloth or inspissated pus
DIAGNOSIS - Clinical examination/anterior rhinoscopy TREATMENT -removal
NASAL POLYP • SIMPLE NASAL POLYP • - allergic rhinitis • - vasomotor rhinitis • - inflammatory: • - acute • - chronic non specific • - chronic specific • - mixed infective allergic rhinitis
2. NEOPLASTIC • Benign • Malignant • Site of origin: • - ethmoidal sinuses incidence at any age • - antral more commonly in children & young adult
NASAL NEOPLASMS • - primary nasal cavity • - secondary from paranasal sinuses, nasopharynx • DIAGNOSIS • clinical examination/rhinoscopy • histopathological examination • TREATMENT • based on: • -the symptoms, signs • -histopathological test results
MOUTH & PHARYNX • CONGENITAL ANOMALIES • THYROGLOSSAL CYSTS • - between the suprasternal notch and the foramen • caecum • 2. STENOSIS OF THE PHARYNX • - in the nasopharyngeal isthmus • 3. WEB OR STRICTURE OF THE PARYNX • - rare • - in post cricoid region of the laryngopharynx
INFLAMMATION OF THE PHARYNGEAL LIMPHOID TISSUE • nasopharyngeal tonsil hypertrophic • physiologic condition at the 3-7 years old DIAGNOSIS -clinical examination posterior rhinoscopy -X-ray film TREATMENT -surgical
ACUTE RETROPHARYNGEAL ABSCESS Abscess lies between the buccopharyngeal and pre Vertebral fasciae • AETIOLOGI • Suppuration in the retropharyngeal lymph-gland • Infection spreading from naso & oropharynx • TREATMENT • -incision of the abscess • -systemic disinfection • -tracheostomy
TUMOURS OF THE NASOPHARYNX INCIDENCE - male more common than female - age: -8-50 years old -18-20 commonest TYPE OF TUMOURS - juvenile nasopharyngeal fibroma - juvenile nasopharyngeal angiofibroma
SQUAMOUS CELL CARCINOMA - the commonest type - varying degrees of differentiation - fossa Russenmulleri is a common site DIAGNOSIS - symptoms & signs - posterior rhinoscopy - biopsy & histopathological examination
TREATMENT - based on the stage & metastatic spreading - tracheostomy - irradiaton - surgery - combination of both
TUMOURS OF THE LARYNGOPHARYNX - especially inferior group - between the upper border of the cricoid cartilage and oesophageal opening - female more common (90%) DIAGNOSIS - radiography & endoscopy - biopsy & histopathological examination
TREATMENT - based on the stage & metastatic spreading - tracheostomy - irradiaton - surgery - combination of both
LARYNX CONGENITAL ABNORMALITIES LARINGOMALACIA - tissue of the larynx are flabby - congenital web of the larynx - fibrous tissue stroma covered by epithelium - usually in the anterior half of glottis - atresia may be complete DIAGNOSIS - endoscopic examination
Choanae Tonsilla palatina Epiglottis Aditus laringeus
TREATMENT • no treatment in the milder form • (just hoarseness) • - tracheostomy severe stridor & dyspnoea • - web excision
TRAUMATIC CONDITION - compression (closed) injury - penetrating (open) injury DIAGNOSIS - the history & physical signs - radiography TREATMENT - intubation/tracheostomy - systemic disinfection - repair the effect of trauma
BURNS AND SCALDS AETIOLOGY - inhalation of irritant fumes or gases - swallowing of corrosive fluids - inhalation of steam DIAGNOSIS - the history & physical signs TREATMENT - rest - steroid - systemic desinfection - tracheostomy or laryngotomy
INHALED FOREIGN BODIES - organic or anorganic foreign bodies DIAGNOSIS - the history & physical signs - radiography - endoscopy TREATMENT - removal by direct laryngoscopy - tracheostomy or laryngotomy - systemic disinfection, anti inflammation drug
INFLAMMATION OF THE LARYNX ACUTE SIMPLE LARYNGITIS IN CHILDREN - most serious than in adult - lymphatic supply is richer - the submucosa more likely to be infected - neuromuscular is more easily spasm - less able to expel the secretions by coughing
TREATMENT - rest in bed - systemic disinfection - oxygen - nasotracheal tube - tracheostomy - laryngotomy
OTHER DISEASE - acute epiglottitis - acute laryngotracheobronchitis - diphtheritic laryngitis
NEOPLASM OF THE LARYNX • BENIGN NEOPLASM • Epithelial tumours: • -single papilloma of the larynx • -multiple papillomata • 2. Connective tissue tumours: • -fibroma of the vocal cord • -chondroma • -angioma