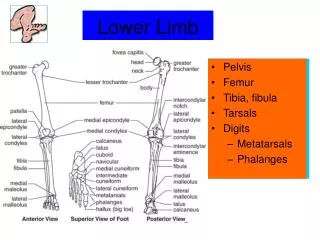
Pediatric Limb Deficiency
Pediatric Limb Deficiency. Ramona M.Okumura, C.P./L.P. Clinical Prosthetist Senior Lecturer, Division of Prosthetics Orthotics Department of Rehabilitation Medicine School of Medicine University of Washington. Introduction. small number born with or acquiring a limb deficiency

Pediatric Limb Deficiency
E N D
Presentation Transcript
Pediatric Limb Deficiency Ramona M.Okumura, C.P./L.P. Clinical Prosthetist Senior Lecturer, Division of Prosthetics Orthotics Department of Rehabilitation Medicine School of Medicine University of Washington
Introduction • small number born with or acquiring a limb deficiency • vast majority have no known etiology • child’s changing developmental capabilities continuously alter the team treatment plan • must keep the doors open for long-term goals and yet provide for optimal functioning • successful outcome depends on treatment of the whole family • very pleasant clients which usually do very well in a healthy family unit
Objectives • Be able to classify Limb Deficiencies • Identify particular management issues • Know how often to review the prescription as the child grows • Predict a functional outcome
Epidemiology • Incidence estimated at 4 per 10,000 births • Congenital 60% to Acquired 40% • Male : Female • Congenital 1.2:1 • Acquired 3:2 • Left : Right • 2:1 in unilateral UE Transverse Deficiency
EpidemiologyCommon presentations Unilateral transverse deficiency of the forearm middle third
EpidemiologyCommon presentations Unilateral conversion by ankle disarticulation for longitudinal fibular deficiency
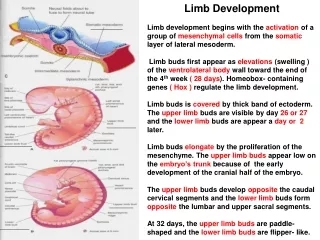
Embryology • Limbs form 4-7 weeks gestation • Proximal to distal in sequence • Upper limb develops slightly ahead of the lower limb • Simultaneously with organ development • Associated with Radial deficiency
Etiology ofCongenital Deficiencies • Environmental • Genetic
Environmental Etiology • precise origin unknown in the majority of cases
Environmental Etiology • precise origin unknown • Speculate Vascular causes particularly some kind of Thromboembolism
Environmental Etiology • precise origin unknown • Speculate Vascular/Thromboembolism • Mechanical: Amniotic Bands or Streeter’s dysplasia in which multiple limbs are involved
Environmental Etiology • precise origin unknown • Speculate Vascular/Thromboembolism • Mechanical: Amniotic Bands • Maternal: • diabetes mellitus • intrauterine infection
Environmental Etiology • precise origin unknown • Speculate Vascular/Thromboembolism • Mechanical: Amniotic Bands • Maternal causes • Pharmaceutical: • Thalidomide only proven drug • Others suspected, no convincing evidence
Genetic Etiology Chromosomal: ex. Turner’s syndrome XXX
Genetic Etiology Single Gene • Autosomal Dominant: Longitudinal tibial deficiency
Genetic Etiology Single Gene • Autosomal Dominant • Autosomal Recessive: TARThrombocytopenia Absent Radius
Etiology ofAcquired Deficiencies Trauma 67% especially trains and lawn mowers
Etiology ofAcquired Deficiencies • Disease33% majority caused by malignancy, particularly 12-21 years of age
Etiology ofAcquired Deficiencies Surgical conversion for congenital limb deficiency
Classification ofCongenital Limb Deficiency International Organization for Standardization (ISO) restricted to skeletal radiological deficiency
ISO Classification ofCongenital Limb Deficiency Transverse deficiency: no skeletal elements present distally • Name the level of the portion of the limb involved (Upper Arm) • State the portion where the absence occurs (“middle third” or “total”)
ISO Classification ofCongenital Limb Deficiency Left Transverse deficiency: • Forearm • middle third
ISO Classification ofCongenital Limb Deficiency Longitudinal deficiency: skeletal elements present axially or distally • Name the bones involved • State partial or total absence
ISO Classification ofCongenital Limb Deficiency Right Longitudinal deficiency: • Fibula total • Tarsals partial • Rays 3,4,5 total
Frantz and O’Rahilly Classification Congenital Limb Deficiency • terminal or intercalary • transverse or paraxial • complete or incomplete • additional terms • amelia total absence of the limb involved • hemimelia partial absence of the limb involved • phocomelia absence of the long bones
Classification ofAcquired Limb Deficiency Through long bones • Upper Extremity • Transradial = Below Elbow (BE) • Transhumeral = Above Elbow (AE) • Lower Extremity • Transtibial = Below Knee (BK) • Transfemoral = Above Knee (AK) • Limb Salvage and Turnplasty (Van Ness)
Classification ofAcquired Limb Deficiency Through the joint: Name the joint + “Disarticulation” • Upper Extremity: Wrist Disarticulation, etc. • Lower Extremity: Ankle Disarticulation, etc.
Clinical PrinciplesTreatment goals • Healthy body image • Maintain choice for prosthetic options • Optimal function
Clinical PrinciplesGeneral considerations • Team approach • Developmental focus • Return appointments • 3-4 months to eval prosthetic fit & function • Annually for team to assess developmental needs
Clinical PrinciplesPsychosocial Support • Clients need to meet others with similar presentations • Guilt and associated familial problems • Give child control and decision making opportunities • Genetic counseling should be provided to both the child and parents
Clinical PrinciplesSurgical Planning • Timing for congenital conversions
Clinical PrinciplesSurgical Planning • Timing • Growth plate considerations
Clinical PrinciplesSurgical Planning • Timing • Growth plate considerations • Overgrowth with long bone transections
Clinical PrinciplesSurgical Planning • Timing • Growth plate considerations • Overgrowth • Planning for multiple surgical procedures
Clinical Principles OT and PT • When infants, we must train parents and caregivers • Children need minimal “training” instead need opportunity
Clinical Principles Prosthetic designs • Endoskeletal vs. exoskeletal • Flexible vs. rigid • Growth adjustable designs • Socks when applicable can allow for growth • For unilateral deficiencies, legs are used, but arms often rejected • Recreation
Clinical PrinciplesLE Prosthetic Considerations Wearing guidelines • Fit when pull the stand and cruising (9-12 months)
Clinical PrinciplesLE Prosthetic Considerations Foot/Ankle • Toddler gait • Lacks heel strike • Wide base of support
Clinical PrinciplesLE Prosthetic Considerations Child’s gait • more normal gait • benefit from dynamic foot/ankle
Clinical PrinciplesLE Prosthetic Considerations Knee • Toddler has fixed/locked knee • Some centers experimenting with a free knee
Clinical PrinciplesLE Prosthetic Considerations Knee • Toddler has fixed/locked knee • At 3 y.o. temporary reduction of Knee ROM while learning
Clinical PrinciplesLE Prosthetic Considerations Hip • uses alignment stability
Clinical PrinciplesUE Prosthetic Considerations Wearing guidelines • 3 mos for supine grasp • “Fit when sit” • Best before 12 mos. • Common periods for rejection • Unilaterals functional without prosthesis, but more receptive learners than adults
Clinical PrinciplesUE Prosthetic Considerations Grasp • Passive as an infant for gross grasp
Clinical PrinciplesUE Prosthetic Considerations Grasp • Active when developmentally “ready” and able to “understand” grasping function (18-24 months)
Clinical PrinciplesUE Prosthetic Considerations Grasp • Electric switch control can provide active control at an earlier age
Clinical PrinciplesUE Prosthetic Considerations Elbow • Fixed for sitting balance as an infant
Clinical PrinciplesUE Prosthetic Considerations Elbow • Fixed as an infant • Passive friction for toddler • Active locking at 3 years old
Clinical PrinciplesUE Prosthetic Considerations High level prosthetic function poor substitute and often rejected
Special Case Discussion Proximal Femoral Focal Deficiency (PFFD) • Aitken A or B