Download
1 / 82
830 likes | 919 Views
Learn about Diagnosis, Intervention, Evaluation, and Documentation in nutrition care process. Identify risk factors, plan interventions, evaluate outcomes, and document effectively. Gain insights into PES statements and interdisciplinary collaboration.

E N D
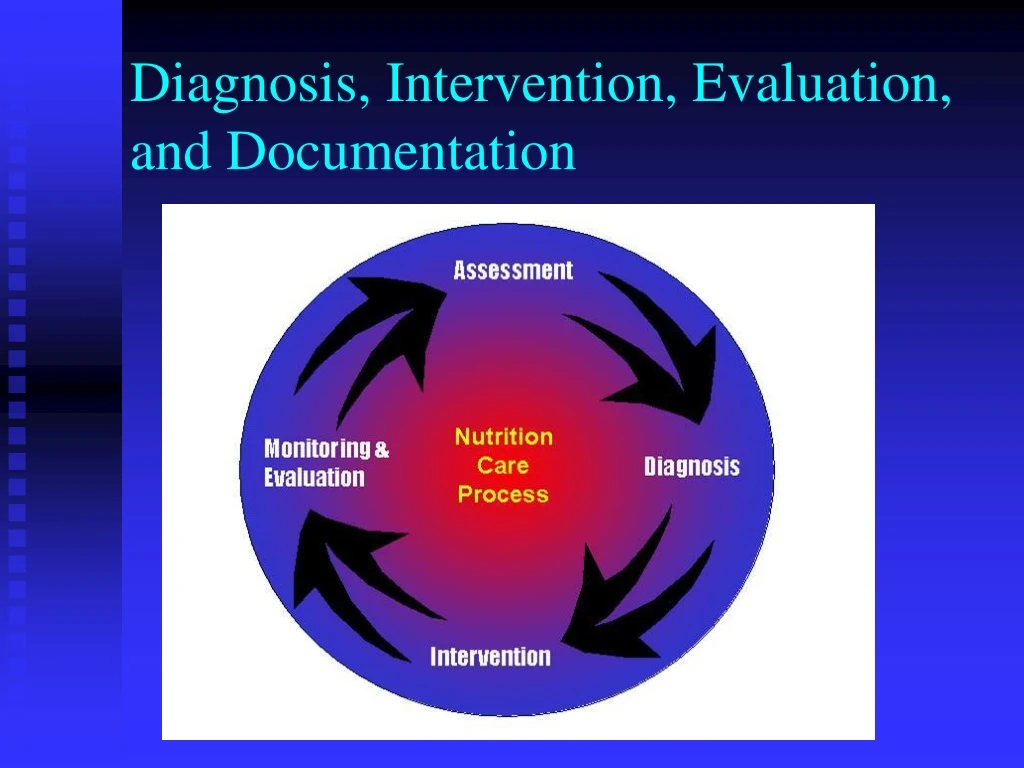
Ø ADA NUTRITION CARE PROCESS AND MODEL Screening & Referral System Ø Identify risk factors Ø Use appropriate tools and methods Ø Involve interdisciplinary collaboration Nutrition Diagnosis Ø Identify and label problem Nutrition Assessment Ø Determine cause/contributing risk Ø Obtain/collect timely and factors appropriate data Ø Cluster signs and symptoms/ Ø Analyze/interpret with defining characteristics evidence - based standards Ø Document Document Relationship Between Patient/Client/Group Nutrition Intervention Dietetics & Ø Plan nutrition intervention · Professional Formulate goals and determine a plan of action Implement the nutrition intervention Ø · Care is delivered and actions Nutrition Monitoring and - are carried out Evaluation Ø Documen t Ø Monitor progress Ø Measure outcome indicators Ø Evaluate outcomes Ø Document Outcomes Management Sys tem Ø Monitor the success of the Nutrition Care Process implementation Ø Evaluate the impact with aggregate data Ø Identify and analyze causes of less than optimal performance and outcomes Ø Refine the use of the Nutrition Care Process
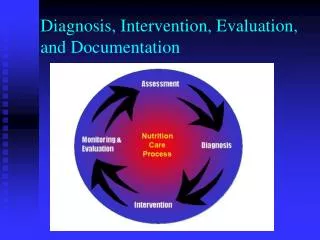
Nutrition Assessment Leads to Nutrition Diagnosis • Nutrition Assessment • Nutrition Diagnosis • Nutrition Intervention • Nutrition Monitoring and Evaluation
PES Statement • Problem: nutrition diagnosis label • Etiology: the focus of the intervention • Signs and symptoms: change when nutrition problems are successfully treated; the focus of monitoring and evaluation
Problem (Diagnostic Label) Falls into three general domains: • Intake (NI) • Excessive or Inadequate intake compared to requirements • Clinical (NC) • Medical or physical conditions that are outside normal • Behavioral/environmental (NB) • Knowledge, attitudes, beliefs, physical environment, access to food, food safety
Etiology • Etiology (Cause/Contributing Factors) • Related factors that contribute to problem • Identifies cause of the problem • Helps determine whether nutrition intervention will improve problem • Linked to problem by words “related to” (RT) • Note: etiology may not always be clear
Etiology • Etiology (Cause/Contributing Factors) • Excessive energy intake (problem) “related to” regular consumption of large portions of high-fat meals (etiology)… • Swallowing difficulty (problem) RT recent stroke (etiology)… • Involuntary wt gain RT decrease in exercise…
Diagnostic Labels Can Be Problems or Etiologies • Inadequate energy intake (NI-1.4) related to food-nutrition knowledge deficit (NB-1.1) • Food-nutrition knowledge deficit (NB-1.1) related to lack of previous nutrition education • Involuntary weight loss (NC-3.2) related to inadequate energy intake (NI-1.4) • Inadequate oral food-beverage intake (NI-2.1) related to swallowing difficulty (NC-1.1)
Signs and Symptoms • Signs/Symptoms (Defining characteristics) • Evidence that problem exists • Linked to etiology by words “as evidenced by” • Evaluation and monitoring of effectiveness of intervention is done by reviewing signs and symptoms
Nutrition Dx with S/S • Excessive energy intake (NI-1.5) (P) • “related to” regular consumption of large portions of high-fat meals (E) • “as evidenced by” diet history & 12 lb wt gain over last 18 mo (Signs)
Nutrition Assessment Identifies Etiology and S/S • Problem: excessive energy intake • Etiology: reviewing the diet history, we learn that • Patient eats in fast food restaurants 2x day • Patient supersizes portions because it’s a bargain • Patient has only 15 minutes for lunch
Etiology Guides Intervention! • The clinician determines what the intervention is by looking at the root cause of the nutrition problem. • If the cause of excessive energy intake is eating frequently in fast food restaurants, how would you intervene?
PES Statements • Excessive fat intake (NI-5.6.2) related to high intake of fried foods and bakery goods as evidenced by diet history and hyperlipidemia • Excessive energy intake (NI-1.5) related to high intake of fried foods and snack items as evidenced by diet history and BMI • Food/nutrition related knowledge deficit (NB-1.1) related to lack of education on cholesterol lowering diet as evidenced by history and patient self-report
Nutrition Diagnosis Statement Should Be • Clear, concise • Specific • Related to one problem • Accurate – related to one etiology • Based on reliable, accurate assessment data
Evaluating Your PES Statement • There are no right or wrong PES statements • But some are better than others
Evaluating Your PES Statement • Can the RD resolve or improve the nutrition diagnosis? • Can your intervention address the etiology and thus resolve it or improve the problem? • Or can your intervention address the signs and symptoms?
Evaluating Your PES Statement • Ex: Inadequate energy intake related to decreased taste perception as evidenced by diet history, medical dx and weight loss of 10 lb. during cancer tx • Cannot treat the etiology (decreased taste perception) but can treat S&S by recommending foods with stronger flavors
Evaluating Your PES Statement • Altered nutrition-related labs related to GI bleed as evidenced by medical hx and decreased hgb/hct in medical record • Labs likely won’t improve until GI bleed is addressed; the etiology is not a nutritional deficit • CAN address inadequate intake of iron, copper, B12, protein, etc.
Evaluating Your PES Statement • When all things are equal and there is a choice between two nutrition diagnoses from different domains, consider the Intake domain diagnosis as the one more specific to the role of the RD • Instead of Altered nutrition-related labs related to GI bleed as evidenced by medical hx and decreased hgb/hct in medical record • Consider Inadequate intake of iron (NI-5.10.1) related to increased needs due to GI bleed as evidenced by medical history, blood count, diet history, and serum ferritin
Evaluating Your PES Statement • Will measuring the signs and symptoms tell you if the problem is resolved or improved? • Ex: If nutrition dx is excessive energy intake, can do another diet history at next visit and see if intake has changed; can also check weight
NCP Example: Long Term Care • 85 y.o. resident of LTC facility has lost >10% weight in the last 6 months • Medical workup negative • Oral supplement is ordered but patient continues to lose weight • Nutrition professional is consulted for enteral feeding recommendations
NCP Example: LTC • On assessment, it is found that patient’s teeth no longer fit and she cannot chew regular meats and vegetables; patient is storing oral supplement in drawer as she worries about the cost
NCP Example: LTC • Diagnosis: Inadequate energy intake (NI-1.4) related to poorly fitting dentures and hoarding of oral supplement as evidenced by observation and pt interview
Etiology Guides Intervention • Intervention: Nutrition professional orders dental consult (RC-1.3) to reline dentures and chopped diet (ND-1.2); puts resident on Medpass supplement (ND-3.1.1)
ADA’s Nutrition Care Process Steps • Nutrition Assessment • Nutrition Diagnosis • Nutrition Intervention • Nutrition Monitoring and Evaluation
Nutrition Intervention • Should be targeted at etiology • If not etiology, then signs and symptoms
Nutrition Interventions Four categories of nutrition interventions: • Food and/or nutrient delivery (ND) • Nutrition education (E) • Nutrition counseling (C) • Coordination of nutrition care (RC)
Food and/or Nutrient Delivery • Meals and snacks (ND-1) • Enteral/parenteral nutrition (ND-2) • Medical food supplements (ND-3.1) • Vitamin and mineral supplement (ND-3.2) • Bioactive substance supplement (ND-3.3) • Feeding assistance (ND-4) • Feeding environment (ND-5) • Nutrition-related medication management (ND-6)
Nutrition Education (E) • Initial/brief nutrition education (E-1) • E.g. survival skills on discharge • Comprehensive nutrition education (E-2) • Purpose • Recommended modifications • Result interpretation • Other Note: Education is appropriate for food and nutrition-related knowledge deficit. If the client knows the content, more education probably won’t help
Nutrition Counseling (C) • Theory or approach • Strategies • Phase
Nutrition Counseling: Theory or Approach The theories or models used to design and implement an intervention; provide a research-based rationale for designing and tailoring nutrition interventions • Cognitive-behavioral therapy (C-1.2) • Health belief model (C-1.3) • Social learning theory (C-1.4) • Transtheoretical Model/Stages of Change (C-1.5) • Other (C-1.6)
Motivational interviewing (C-2.1) Goal setting (C-2.2) Self-monitoring (C-2.3) Problem solving (C-2.4) Social support (C-2.5) Stress management (C-2.6) Stimulus control (C-2.7) Cognitive restructuring (C-2.8) Relapse prevention (C-2.9) Rewards/contingency mgt (C-2.10) Other Nutrition Counseling: Strategies* *Selectively applied evidence-based method or plan of action designed to achieve a particular goal
Coordination of Care (RC) • Coordination of other care during nutrition care (RC-1) • Team meeting • Referral to RD • Collaboration with other providers • Referral to community agencies/programs • Discharge and transfer of nutrition care to new setting/provider (RC-2) • Collaboration • Referral to community agencies/programs
ADA’s Nutrition Care Process Steps • Nutrition Assessment • Nutrition Diagnosis • Nutrition Intervention • Nutrition Monitoring and Evaluation
Nutrition Monitoring and Evaluation • Monitor progress and determine if goals are met • Identifies patient/client outcomes relevant to the nutrition diagnosis and intervention plans and goals • Measure and compare to client’s previous status, nutrition goals, or reference standards
Nutrition Outcomes – 4 Categories • Nutrition-Related Behavioral and Environmental Outcomes (BE)—Nutrition-related knowledge, behavior, access, and ability that impact food and nutrient intake • Food and Nutrient Intake Outcomes (FI)—Food and/or nutrient intake from all sources • Nutrition-Related Physical Signs and Symptom Outcomes (S)—Anthropomorphic, biochemical, and physical exam parameters • Nutrition-Related Patient/client centered Outcomes (PC)—perception of patient/client’s nutrition intervention and its impact
Nutrition-Related Behavioral and Environmental Outcomes (BE) • Knowledge/beliefs (1) • Behavior (2) • Access (3) • Physical activity and function (4)
Behavior-Environmental Outcomes Domain: Beliefs and Attitudes (BE-1.1) Definition: beliefs/attitudes about and/or readiness to change food, nutrition, or nutrition-related behaviors Potential indicators (BE-1.1) • Readiness to change • Perceived consequences of change • Perceived costs versus benefits of change • Perceived risk • Outcome expectancy • Conflict with patient/family value system • Self efficacy
Beliefs and Attitudes (BE-1.1) Measurement methods or data sources • Patient self-report, client/patient assessment questionnaire or interview Typically used to monitor and evaluate change in the following domains of nutrition intervention: • Nutrition education, nutrition counseling
Beliefs and Attitudes (BE-1.1) Typically used to monitor and evaluate change in the following nutrition diagnoses • Harmful beliefs/attitudes about food- or nutrition-related topics • Not ready for diet/lifestyle change • Inability to manage self-care • Excess or inadequate oral food/beverage, energy, macronutrient, micronutrient, or bioactive substance intake • Imbalance of nutrients • Inappropriate fat foods
Beliefs and Attitudes (BE-1.1) Typically used to monitor/evaluate change in the following nutrition diagnoses (cont) • Inappropriate intake of amino acids • Underweight • Overweight/obesity • Disordered eating pattern • Physical inactivity • Excess exercise
Behavior-Environmental Outcomes Domain: Food and Nutrition Knowledge (BE-1.2) Definition: Level of knowledge about food, nutrition and health, or nutrition-related information and guidelines relevant to patient/client needs
Food and Nutrition Knowledge (BE-1.2) Potential Indicators • Level of knowledge (e.g. none, limited, minimal, substantial, and extensive • Areas of knowledge: • Food/nutrient requirements • Physiological functions • Disease/condition • Nutrition recommendations • Food products • Consequences of food behavior • Food label understanding/knowledge • Self-management parameters
Food and Nutrition Knowledge (BE-1.2) Measurement methods or data sources • Pre and post-tests administered orally, on paper, or by computer • Scenario discussions • Patient/client restate key information • Review of food records • Practical demonstration/test Typically used to monitor and evaluate change in the following domains of nutrition intervention: • Nutrition education, nutrition counseling